
Yasmin Abdul Rashid ( Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Zahra Abdul Ghafoor ( Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Nehal Masood ( Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Talha Mehmood ( Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Safia Awan ( Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Tooba Ansar ( Medical Student, The Aga Khan University Hospital, Karachi, Pakistan. )
Murtaza Mirza ( Medical Student, The Aga Khan University Hospital, Karachi, Pakistan. )
Uzma Abdul Rashid ( Student, University of Maryland, Baltimore County, USA. )
September 2012, Volume 62, Issue 9
Original Article
Abstract
Objectives: To explore the effects of cancer on psychosocial aspects of Pakistani patients and their families, assessing the need for interventions to improve their quality of life.
Methods: A prospective, Cross-sectional study was performed on 200 patients visiting the oncology outpatient facility of AKUH from December 2010 to May 2011 through an interview. Responses were recorded on pre-designed questionnaires including FACT-G QOL (Functional Assessment of Cancer Therapy-General Quality Of Life) component.
Results: Out of the 200 patients 52 (26%) were males and 148 (74%) were females. Mean age was 51.8 ± 14.2 years. Breast cancer accounted for the commonest cancer in females 116 (58%) and lung in males 30 (15%), 100 (50%) patients were currently undergoing chemotherapy. In all 148 (74%) patients were well aware of their diagnosis and were able to cope better and 142 (71%) were well supported by families (majority being financially stable). Major financial impact was found in 42 (21%) cases. Religious/spiritual help was sought by 138 (69%) patients predominantly females- 113 (76%) and 22 (11%) patients consulted a psychiatrist; 20 (94%) subjects of this group felt this intervention was helpful. Responses regarding effect on the patient\\\'s sexual life were poor and 126 (63%) denied answering the question.
Conclusion: In our study one third of cancer patients were found to be depressed mainly affecting those who were receiving multimodality treatment or facing financial issues. Religious help was the main coping strategy for them.
Keywords: Psychosocial aspects, Cancer patients, Coping strategy. (JPMA 62: 905; 2012)
Introduction
Cancer is the second-leading cause of death in the United States, exceeded only by heart diseases.1 Unfortunately, Pakistan has been unsuccessful in sustaining the numerous population-based cancer registries in the past,2 but since the establishment of KCR (Karachi Cancer Registry) and APCR (Aga Khan University Pathology-based Cancer Registry), the cancer database was functional, with a reported increase in the incidence of cancers during the last decade.2
There is considerable evidence suggesting that cancer patients suffer from substantial and long-term psychological distress associated with different forms of cancer and its medical treatment.3 With cancer on dramatic rise in the underdeveloped countries according to the WHO,4 especially in our region,2 physicians involved in treating such patients should be well equipped to deal with the previously undermined consequences of this grave illness.
The burdens that a cancer patient faces not only include deteriorating health, but also a significant decline in the Quality of Life5 and significant working disability.6 Addressing these issues is as important as treatment of the disease itself.
Recurrence of the disease is a constant fear among cancer patients, with the affectees more liable to show poor physical functioning, slower quality-of-life improvement and higher cancer-related distress as compared to patients initially diagnosed with it7 thus requiring an ongoing support system to deal with such circumstances as the disease progresses.8
Psychosocial effects of cancer have been under-studied in Pakistan. One study done with breast cancer survivors in Pakistan revealed common reactions including isolation, aggression, and anger. Religion and family support were the essential coping strategies.9 The increased interest in the quality of care studies over the past two decades10 has translated in an equal interest in its relationship with the Quality of Life, and the effect that treatment brings upon it.11 In this study, we tried to identify the major psychosocial factors involved with the adult cancer population and their effects on the patients\' well-being.
Methodology
This was a cross-sectional descriptive study conducted at the Medical Oncology out-patient clinics of the Aga Khan University Hospital, Karachi. During this study no trial or experimental procedure was carried out. Written informed consent was taken from the patients. The study was started after approval from the ethical review committee of the Aga Khan University.
The study included adult patients, male and female, 18 years and above histologically diagnosed with cancer those who consented to be a part of the project. The patients, who did not consent, did not have cancer as established diagnoses were excluded from the study. Data was collected with especially designed questionnaires, in English and Urdu, both, including variables from previously conducted psychosocial factor studies found in the literature search. It also included a validated Functional Assessment of Chronic Illness Therapy (FACIT) 21 item question set assessing the Physical, Social/Family, Emotional and Functional Well-being of the study subjects. To screen the patients for any depressive symptoms the WHO-5 scale was employed, which is a sensitive and specific screening measure for depression in Primary Care settings12 and those who were found to be in the score ranges of being depressed were assessed using Major Depression Inventory (MDI) another sensitive and specific adjunct confirmatory test to diagnose major depression.13
All the questionnaires were first tested on a pilot of 10 patients from the oncology clinic, 10 patients who came to the family medicine clinic at AKUH, and 10 normal subjects, outside AKUH. The interviews were conducted by trained individuals who either administered the pre-designed questionnaire on the non-reading/uneducated population, recorded their responses or gave the questionnaire to the patients to fill on their own after explaining them. After the pilot, similar technique was used to collect data from 200 patients visiting the medical oncology clinic, AKUH.
A sample size of 200 subjects was required to fulfill the objective of our study at a 95% confidence level. We assumed a 50% of good quality of life, 6% bound-of-error with a power of 80%.
Data entry was conducted by two separate groups of individuals to minimize error using EpiData version 3.1. Each group entered the data independently and then both records were compared to detect data entry errors. If errors were found, details of that study participant were retrieved and the errors were rectified, and there were three such instances. Data was analyzed by using the Statistical Package for Social Sciences version 19.0. Relevant descriptive statistics, frequency and percentage were employed for categorical variables. Mean and standard deviation were computed for quantitative variables. No statistical test of significance was applicable for this descriptive study.
Results
Out of the 200 patients 52 (26%) were males and 148 (74%) were females.
Mean age was 51.8 ± 14.2 years, 150(75%) of the total patient population were married, 50 (25%) single including separated divorcees and widowed patients. Breast cancer accounted for the most common form of cancer in females 116(58%) and lung cancer was mostly prevalent in males 30(15%). Other cancers included Head and Neck cancers, leukaemia, Lymphomas, gynaecological malignancies and gastrointestinal tumours.
Seventy two (36%) patients were found to be clinically depressed on MDI, 110(55%) were not depressed, and were hopeful. 18 (9%) were in denial of their condition.
One hundred (50%) patients were currently undergoing chemotherapy, 4(2%) were undergoing radiotherapy, 12(6%) had been treated surgically, and 58(29%) of patients were under surveillance. Multimodality treatment in combination as surgery, chemotherapy and radiation, surgery and chemotherapy, radiation and chemotherapy, and surgery and radiation were given to 20 (10%) patients. There were 6 (3%) palliative care patients being provided supportive treatment. Of these patients, majority on multimodality treatment were found to be depressed on MDI (Major Depression Inventory) (being 66.7%, 55.5%, 66.7% and 100% respectively for patients undergoing Surgery, chemotherapy and radiation, Surgery and chemotherapy, radiation and chemotherapy, and surgery and radiation) Whereas, patients receiving single treatment modality at the time of their recruitment were mostly hopeful, being 9 (75%), 54 (53.5%) and 4 (100%) for surgery, chemotherapy and radiation respectively. Patients on surveillance numbered 41 (70%) and they were hopeful. Four (80%) patients on supportive care were found to be depressed on the MDI. Denial was also found to be higher among them.
One hundred twelve (56%) cases were diagnosed within the year of their recruitment with 64 (32%) being between 2-5 years from their diagnosis, and 24 (12%) were diagnosed more than 5 years ago at the time of their recruitment in the study. Among these groups depression was higher in patients diagnosed within 1 year, 68 (57%) of them being diagnosed as depressed on MDI. This trend decreased with the passage of time since diagnosis, being 32 (50%) among patients within 1-5 year group, and 7 (29%) in patients who were more than 5 years from the time they were diagnosed, with 15 (63%) of them being hopeful.
One hundred forty eight (74%) patients were aware of the diagnosis and prognosis of their disease, 44 (22%) were unclear of their diagnosis, or the prognosis of their disease. Eight (4%) were unaware of their disease or prognosis. Of the patients, who were aware, 89(60%) were hopeful, whereas 30(67%) who did not know about their disease were depressed on the MDI. Denial was found to be highest among patients who somewhat knew of their disease, with the highest frequency being 2 (25%).
Religious/spiritual help was sought by 138 (69%) patients (predominantly females) (113/ 76%). This was helpful in reducing the anxiety/stress level for 120(87%) of the patients who took such measures, including prayers, meditation and visiting spiritual healers who did not employ any therapeutic/alternative measures.
Twenty two (11%) patients consulted a psychiatrist, and 20 (94%) found this intervention helpful. Two(6%)patients who did not find it helpful had visited either once, or had stopped going to the psychiatrist (one of each). Among the patients who were well aware of their diagnosis and the prognosis of their diseases, 85 (59%) were hopeful and 50 (34%) were depressed and pessimistic.
The major financial burden was mostly borne by patients themselves 50 (25%) and by the patient\\\'s families 113 (56.5%).Twenty eight (14%) were supported by their employers/corporate and 8 (4%) had welfare support. The disease imposed a burden on 42 (21%) patients financially, to the extent of making major changes like selling properties, and breaking financial stores etc. Eighty(40%) had to make moderate changes like lifestyle alteration, downgrading cars; changing houses etc. Sixty eight (34%) were not affected by the financial burden of their disease. Of the financially non-stricken population, 24 (35%) were found to be depressed on the MDI, however, 38 (48%) of the moderate financially affected, and 27 (64%) of majorly financially affected individuals were found to be depressed on the MDI.
The FACIT questionnaire revealed significant items (responses that were 4 and above out of 5) mentioned in Table 1-2.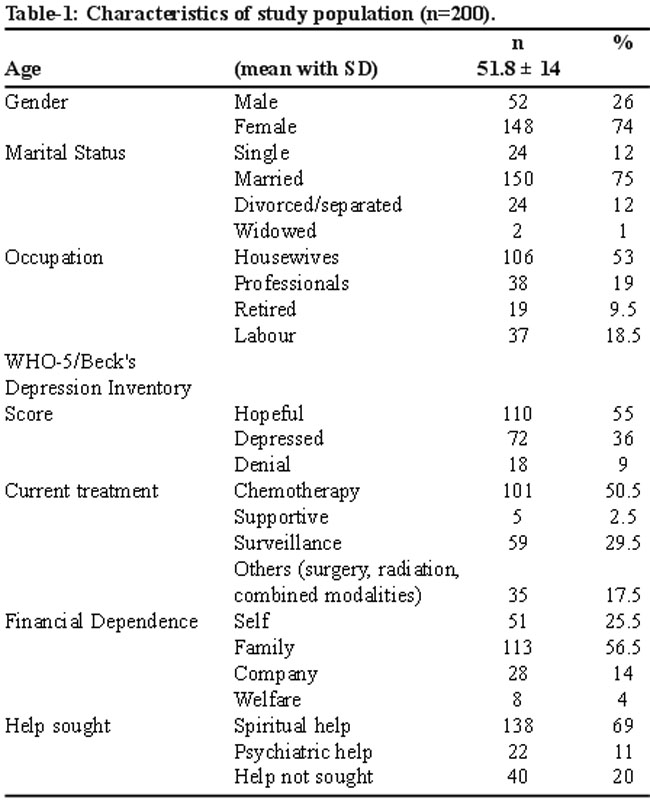
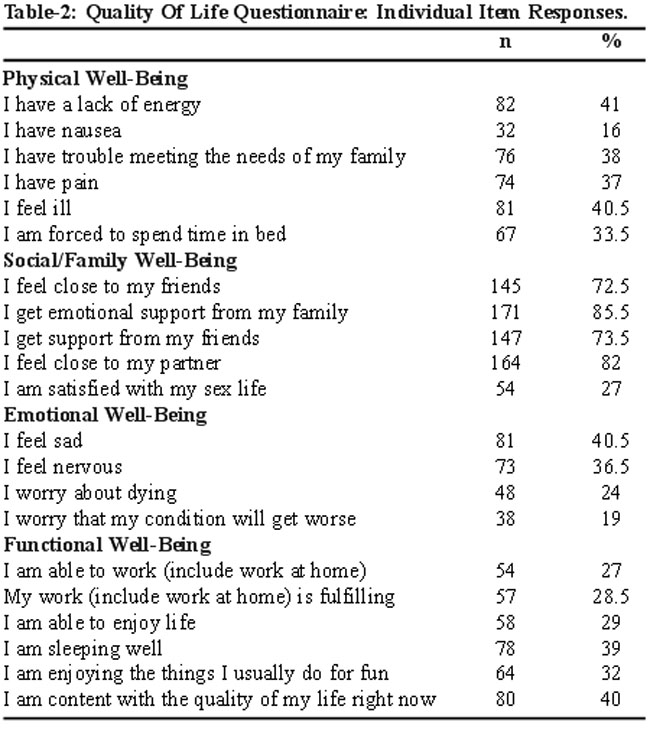
It assessed physical, social/family, emotional and functional wellbeing, which included variables as: Lack of energy and body pain, and their effect on functionality, meeting family needs, closeness with partners, friends and family, sexual contentment, feelings of sadness and despair, and thoughts about worsening/recurring cancer, and death.
Discussion
Cancer is a serious and widespread disease which not only confers greater mortality, 13 but also adversely affects the life of the patient. This contributes to an extraordinary burden of health in the under-developed world, and continues to rise as a major cause of early mortality. As much as 70% precious Years of Life are Lost (YLLs) due to the burden of Cancer.15
People react in many ways to the news of being diagnosed with Cancer, and may feel shocked, be in denial of the situation9 and conceal the evidence of its existence, or choose to deal with their condition by not treating it at all. However cancer subjects people to tested apparatus of clinical knowledge and their progress is mapped accordingly. This process, however clinically fitting, involves upheavals in the lives of the patients and the studies conducted before have conferred evidence to this statement.14
This study was undertaken to understand psychosocial needs of the patients diagnosed with cancer in our part of the world. Interviews with 200 respondents revealed that this was a difficult diagnosis and affected them in ways more than oncologists treat them for. The screening for depression employing the WHO-5 questionnaire and MDI (Major Depression Inventory) not only revealed depression as a common finding among the cancer patients, but also highlighted an easily treatable condition bringing down their quality of life. Financial burden also proved to be an important factor hindering the well-being of these patients.
Depression although prevalent among all the sub-groups of the study sample was higher in the patients receiving multimodality treatment. There may be a selection bias here, but Oncologists treating such patients should address such causes earlier, and alleviate causes amenable to treatment and bring changes in the quality of life of their patients. Same is also true for patients under surveillance or palliative care, as they too were found to be more depressed when screened. The patients on supportive care warrant earlier diagnosis, because as many as 80% were found to be depressed in our study. They need treatment sooner than later, to improve their already limited disease adjusted life years. Depression is not only a common finding in or study but similar studies on breast cancer patients have also identified it. Other psychosocial factors reduce the imminent quality of life, and are also associated with worse outcomes in mortality, and relapse.16 Improving depression may give patients a better fighting spirit, and hope, not only in their treatment, but possibly in their perception of emotional support. This may be associated with better outcomes17 fewer metastases18 and longer event-free survival.19 The alleviation of depression may also enable the patients to be more socially active, which has been linked with significant disease free survival which was found to increase with an increasing number of hobbies.20 On the other hand, acute and chronic stress, and negativity, loss of social interaction and depression have been linked with lower survival and earlier relapse of disease.21,22
In our study, most people felt they were closer to their friends, family and loved ones as assessed by the FACIT questionnaire. The perceived emotional support has been linked with increased all-cause and cancer related mortality14 and may be improved if factors as depression are addressed earlier. The patients did not adequately answer regarding their sexual life, and were guarded in their responses, most likely due to the taboo associated with conversation regarding one\\\'s sex-life in Pakistan. Only 27% of them responded to the question comfortably. All of them were satisfied with their sex life, and their partners.
The patient\\\'s knowledge of their disease, and prognosis was found to be linked with hope, and better coping in our study. Many a times, the loved ones urge the physicians to keep the patient unaware of a relapse, or at times even the diagnosis. This was associated with greater finding of depression, and denial among patients and hindered their psychological coping, and wellbeing.
It has been only as recent as the advent of the 21st century that researchers turned towards religious, and spiritual domains as potential resources for patients confronted with dilemmas as stressful life events. In Pakistan, religion holds a special and sacred place not only in people\\\'s personal lives but also as a collective societal way of living. This was also found to be true in our study, where religion was a major coping mechanism for our patients confronted with the diagnosis of cancer. Most of the patients who resorted to belief and religion were females, amounting to be as many as 76%, a staggering 87% (n=98) of whom found this intervention to positively affect their outlook towards their disease, and provide a coping mechanism for an overwhelming difficulty. This was not only observed in our study, but has been studied previously, where praying and putting trust in God was the strategy researchers reported to be most often employed, and found most helpful by respondents of their sample in coping with the stress of cancer survival.15
The diagnosis of cancer has a daunting financial implication on the residents of a developing country as Pakistan. Many do not opt for treatment, and even among those who do, as in our study, many have to make sacrifices and alter their lives to find adequate treatment of their disease. In the absence of any government, or insurance support, only 4% were on any kind of welfare aid for their treatment. The majority of the patients were those who were either bearing the expenses on their own or they were being helped by their family. Nevertheless, some lifestyle modification was evident in as many as 61% of the patients. Among them, 42 had sold their property, house, car or financial assets as gold, or jewelry to get treatment, and 80 had changed their housing, downgraded their car and taken a loan for their treatment. Such financial disability was also associated with a higher frequency of depression, and clinicians should be aware of such factors to address the possible solutions in time to improve the patients\\\' quality of life.
It is not just the disease, but what one believes to be associated with it, that makes an impact on how patients see themselves in a disease spectrum of cancer, and how that affects their psychosocial well-being. No matter what stage the patient is at, or what the intent of treatment is, psychological and social issues are omnipotent in all sub-groups of observed study samples. This study points towards the need for addressing these as vigilantly as oncologists treat other key issues as this may improve the quality of life in cancer patients, helping them make the most of their already limited effective life years.
Conclusion
In this study one third of cancer patients were found to be depressed. Patients on multimodality treatment or in whom treatment led to major financial impact were more affected by depression. Religious/spiritual help was found as main coping mechanism for patients to reduce their anxiety/depression.
Future Directions:
Doctors and nurses need to be trained in dealing with psychosocial dilemmas of cancer patients. Screening for depression should be carried out earlier while treating these patients and professional counselors should be part of the oncology team. Given the economic dynamics of the developing world, it is also pertinent to build systems of financial support to bring improvement in their quality of life.
Acknowledgments
Adnan Hussain and Mahwish Kamran are gratefully acknowledged for helping in development of the questionnaire.
References
1. National Cancer Institute. SEER Cancer Statistics Review. (Online) 1975-2007, (Cited 2011 August 17). Available from URL: http://seer.cancer.gov.
2. Bhurgri Y, Bhurgri A, Nishter S, Ahmed A, Usman A, Pervez S, et al. Pakistan - Country Profile of Cancer and Cancer Control 1995-2004. J Pak Med Assoc 2006; 56: 123-30.
3. Rehse B, Pukrop R. Effects of psychosocial interventions on quality of life in adult cancer patients: meta analysis of 37 published controlled outcome studies. Patient Educ Couns 2003; 50: 179-86.
4. Ad Hoc committee oh Health research Relating to Future Intervention Options. Summary of Investing in Health Research and Development, World Health Organization, Geneva: Switzerland; 2005.
5. Montazeri A. Health-related quality of life in breast cancer patients: a bibliographic review of the literature from 1974 to 2007. J Exp Clin Cancer Res 2008; 27: 32.
6. Short PF, Vasey JJ, Belue R.Work disability associated with cancer survivorship and other chronic conditions. Psychooncology 2008; 17: 91-7.
7. Yang HC, Thornton LM, Shapiro CL, Andersen BL. Surviving recurrence: psychological and quality-of-life recovery. Cancer 2008; 112: 1178-87.
8. Donovan KA, Taliaferro LA, Alvarez EM, Jacobsen PB, Roetzheim RG, Wenham RM. Sexual health in women treated for cervical cancer: characteristics and correlates. Gynecol Oncol 2007; 104: 428-34.
9. Banning M, Hafeez H, Faisal S, Hassan M, Zafar A. The impact of culture and sociological and psychological issues on Muslim patients with breast cancer in Pakistan. Cancer Nurs 2009; 32: 317-24.
10. Van der Waal MAE, Casparie AF, Lako CJ. Quality of care: a comparison of reference between medical specialists and patients with chronic diseases. Soc Sci Med 1996; 42: 643-9.
11. Rosser R. The history of health-related quality of life in 10 1/2 paragraphs. J R Soc Med 1993; 86: 315-8.
12. Primack BA. The WHO-5 wellbeing index performed the best in screening for depression in primary care. ACP J Club 2003; 139: 48.
13. Bech P, Rasmussen NA, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J Affect Disord 2001; 66: 159-64.
14. Saegrov S, Halding AG. What is it like living with the diagnosis of cancer? Eur J Cancer Care Engl 2004;13: 145-53.
15. Murthy NS, Nandakumar BS, Pruthrish S, George PS, Mathew A. Disability adjusted life years for cancer patients in India. Asian Pac J Cancer Prev 2010; 11: 633-40.
16. Falgas ME, Zarkadoulia EA, Ionnidou EN, Peppas G, Christodoulocy Rafailidis PI. The effect of psychosocial factors on breast cancer outcome: a systematic review. Breast Cancer Res 2007; 9:R44 (doi:10.1186/bcr1744).
17. Greer S, Morris T, Pettingale KW. Psychological response to breast cancer: effect on outcome. Lancet 1979; 2: 785-7.
18. Levy SM, Lee J, Bagley C, Lippman M. Survival hazards analysis in first recurrent breast cancer patients: seven-year follow-up. Psychosom Med 1988; 50: 520-8.
19. Hislop TG, Waxler NE, Coldman AJ, Elwood JM, Kan L. The prognostic significance of psychosocial factors in women with breast cancer. J Chronic Dis 1987; 40: 729-35.
20. Tominaga K, Andow J, Koyama Y, Numao S, Kurokawa E, Ojima M, Nagai M. Family environment, hobbies and habits as psychosocial predictors of survival for surgically treated patients with breast cancer. Jpn J Clin Oncol 1998; 28: 36-41.
21. Maddineni SB, Lau MM, Sangar VK. Identifying the needs of penile cancer sufferers: a systematic review of the quality of life, psychosexual and psychosocial literature in penile cancer. BMC Urol 2009; 9: 8.
22. Jensen MR. Psychobiological factors predicting the course of breast cancer. J Pers 1987; 55: 317-42.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: