
Majida Khan ( Sindh Institute of Reproductive Medicine (SIRM) Karachi, Pakistan. )
Shaheen Zafar ( Sindh Institute of Reproductive Medicine (SIRM) Karachi, Pakistan. )
Serajuddaula Syed ( Sindh Institute of Reproductive Medicine (SIRM) Karachi, Pakistan. )
September 2012, Volume 62, Issue 9
Original Article
Abstract
Objective: To assess the survival of freezing cleaved human embryos through vitrification.
Methods: The prospective study was conducted at the Karachi-based Sindh Institute of Reproductive Medicine between June 2008 and June 2009. The cryopreservation of embryos being a new technology in Pakistan, only 19 couples, picked through convenience sampling, comprised the study population. The couples were treated for infertility by in virto fertilisation (IVF) or intracytoplasmic sperm injection (ICSI); 125 surplus embryos were vitrified. Subsequently, 15 embryos were thawed, and transferred in a controlled cycle. SPSS version 11 was used for statistical analysis.
Result: After the surplus embryos were vitrified and subsequently thawed and transferred, the survival of the embryos was assessed by the number of blastomeres that were intact. The overall embryo survival rate was (14/15) 93.33%.
Conclusion: Vitrification is a simple procedure that requires less time and is likely to become safer and more cost-effective with time. Survival rate after thawing and preserving is high, but comparative success rates in terms of pregnancy and taking-home-baby rates are yet to be established in Pakistan.
Keywords: In vitro fertilization, Assisted reproduction, Embryo. (JPMA 62: 887; 2012).
Introduction
The major developments in cryopreservation technology have mirrored the rapid expansion of reproductive technology over the past 2 decades and it has become an integral part of assisted reproduction.1 Many cryopreservation procedures have been applied to oocytes, embryos, sperm, ovarian and testicular tissue.2 It provides an opportunity for patients to have more than one attempt following an ovarian stimulation cycle, thereby decreasing the exposure of patients to exogenous gonadotrophins and improving cumulative pregnancy rates.3
Regarding cryopreservation of human gametes, the history stretches back more than 200 years. The first recorded experiment in 1776 involved the cooling followed by successful re-warming of spermatozoa frozen in snow. Since then, huge advances have been made. Two basic techniques have been employed for the cryopreservation of cells: controlled slow-rate freezing and vitrification.4 Each of them is currently applied to human gametes and embryos. Since after the publication of the first biochemical and clinical pregnancies with the frozen-thawed human embryos5,6 in the early 1980s, slow-freezing remains the most commonly used method of cryopreservation in human in vitro fertilisation laboratories around the world,4 but it may result in intra-cellular and extra-cellular crystallisation.
The introduction of vitrification and rapid freezing techniques is gaining widespread recognition and may become the method of choice. The first report of live birth following the vitrification of oocyte came from 1999 in Bologna.1 It is an ultra-rapid method of cryopreservation whereby the embryo is transitioned from 37°C to -196°C in <1 second, resulting in extremely fast rates of cooling (>10,000°C/min). The cells and tissues are placed directly into the cryoprotectants and after only a very short period of equilibrium, the cells are plunged rapidly into liquid nitrogen at a temperature of -196°C. A glass-like solidification occurs soon afterwards. The early development of vitrification involved the use of long pre-equilibration procedures. Improved methods resulted from the use of mixtures of penetrating and non-penetrating solutes that were non-toxic and had a range of cooling rates.4 Recent studies have reported increasingly successful clinical results with vitrification.7,8
Vitrification as a cryopreservation method has many primary advantages and benefits. For instance, there is no ice crystal formation because of increased speed of temperature conduction, which provides a significant increase in cooling rates. This permits the use of less concentrated cryoprotectant agents so that the toxic effect is decreased. Additionally, chilling injuries are considerably reduced. It is relatively simple, and requires no expensive programmable freezing equipment.1 Also, it can be performed by only one embryologist without the use of any costly equipment and within a few minutes.7
To analyse the cellular effect of the cryopreservation method, pyruvate uptake needs to be measured in embryo post thawing/warming. The early embryo predominantly uses pyruvate for metabolism; so measuring the amount of pyruvate consumed by the embryo gives an indication of the embryonic health. Pyruvate uptake by embryos after vitrification is significantly higher than that after slow-freezing.4
To date, the \\\'universal\\\' vitrification protocol has yet to be defined. At which stage embryo cryopreservation can be undertaken most effectively, remains undecided. It is important, therefore, for researchers to achieve more consistent results from existing protocols and thereby establish a standardised vitrification protocol that can be applied for cryopreservation at different developmental stages. Towards this end, it should be noted that vitrification protocols are starting to enter the mainstream of human-assisted reproductive technique (ART). The protocols of ultra-rapid freezing and vitrification are convenient and eliminate the use of expensive controlled-rate freezers, but require validation from more extensive experimental studies. The convenience of vitrification, however, will push the development of this technique to higher levels of clinical efficiency and use.
The Sindh Institute of Reproductive Medicine (SIRM) introduced vitrification in June 2008. As it is a relatively new technique in Pakistan, limited number of cases have been performed only at SIRM.
The aim of this study was, therefore, to assess the efficacy of vitrification on the survival and subsequent development of human cleavage-stage embryos.
Patients and Methods
The \\\'prospective descriptive study\\\' was performed at SIRM between June 2008 and June 2009. It involved 19 couples who were selected by convenience sampling. The couples were treated for infertility by IVF or intracytoplasmic sperm injection (ICSI) or intravaginal culture (IVC). Down regulation and ovulation induction was performed by the administration of gonadotrophin-releasing hormone (GnRH) agonist (Suprefact or Decapeptyl) together with gonadotrophins. Ovulation was triggered by the intramuscular administration of human chorionic gonadotrophin (HCG) 10,000 IU as soon as desirable numbers of follicles of a diameter of 17mm were observed by trans-vaginal ultrasound and with oestradiol concentration corresponding to the number of follicles. Oocyte retrieval under ultrasound guidance was performed 35-36 hours after the trigger. The retrieved oocytes were submitted to IVF, IVC and ICSI procedures. Fresh ejaculated sperm as well as surgically retrieved sperms were used for ART. Intravaginal progesterone (200mg/day) was started 48 hours prior to the embryo transfer, which was done on day two or three. A soft transfer catheter was used for embryo transfer.
A total of 125 surplus embryos (day 2 and 3 cleavage-stage) from 19 couples who underwent IVF, IVC, or ICSI were cryopreserved and subsequently thawed, and transferred in a controlled cycle. All patients were informed and written consent was obtained before the procedure.
Only good-quality embryos having four or more equal-sized and evenly-shaped blastomeres, with <25% fragmentation were cryopreserved by open method. The cryopreserved embryos were subsequently cultured up to the blastocyst stage after thawing/warming.
Embryos were considered to have survived if >50% of the blastomeres were intact or if they had at least three viable cells present at thawing, and showing at least one blastomere divided by 18 hours of post-thawing culture.
The vitrification/warming protocol was performed according to the method described by Kuwayama et al.7 Depending on the case, additional 4-8 cell stage embryos were prepared for vitrification. The embryos (all zygotes from the same patient were treated together for time-saving purposes) were incubated in equilibration solution comprising 7.5% ethylene glycol (EG) and 7.5% dimethyl sulphoxide (DMSO) in Ham\\\'s F-10 media supplemented with 20% patient serum for 5-15 min (depending on the time needed for re-expation of the cell) at room temperature. After an initial shrinkage and recovery, they were then aspirated and placed in to the vitrification solution (15% EG, 15% DMSO, 0.5 M sucrose) in Ham\\\'s F-10 medium supplemented with 20% patient serum for 50-60 sec at room temperature. After having observed cellular shrinkage, embryos were aspirated and placed on the tip of the cryotop. No more than two embryos were placed on each cryotop. Cooling of the embryos was done by direct contact with liquid nitrogen. The cryotops were stored in liquid nitrogen for the period as decided by the patient.
Warming of embryos was performed by placing the cryotop in thawing solution (1.0 M sucrose) for 50-60 sec at room temperature and then into dilution (0.5 M sucrose) for 3 min, both at room temperature. The warmed embryos were placed 4-5 times into washing solution (Ham\\\'s F-10 + 20% serum) before incubation. The intact embryos were cultured in Ham\\\'s F-10 for 24 hours prior to embryo transfer. The embryo quality was scored on the second day before transfer, and survival was assessed morphologically.
Statistical analysis was performed using SPSS version II. Frequency, mean and standard deviation were calculated for quantitative variables.
Results
The female age ranged from 24 to 35 years with a mean of 28.06 ± 3.06 years (Table-1).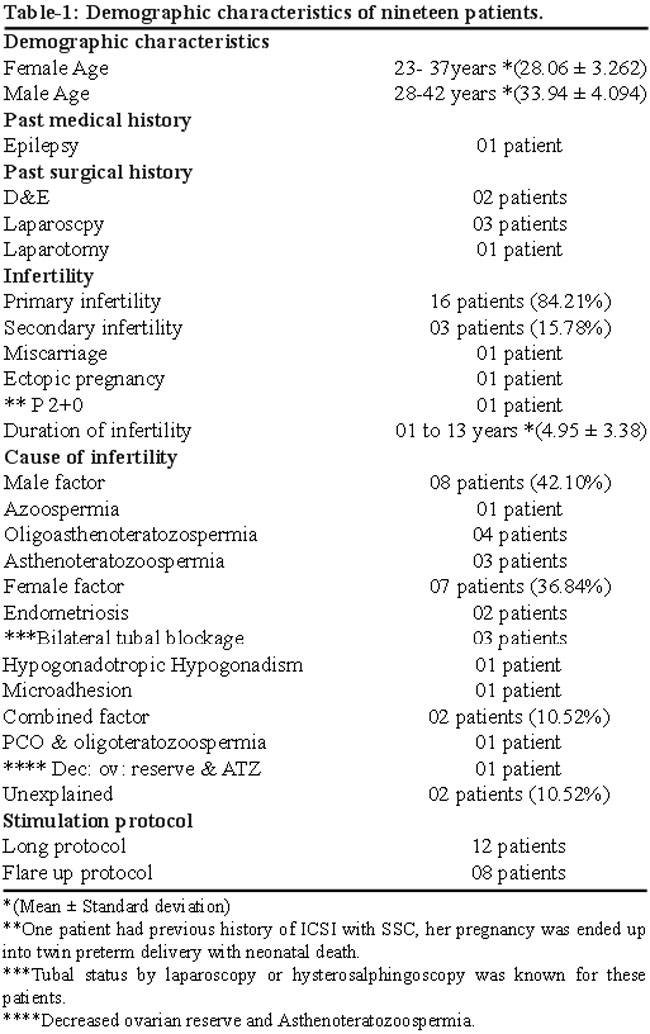
A total of 125 surplus embryos of 19 patients were selected for vitrification. The total number of stimulated cycles was 20; one patient had two cycles attempted as the first cycle had failed. The cause of infertility was either male factor, female factor or combined factor. For 01 azoospermic male patient, sperms were collected by Testicular sperm extraction (TESE).
All cycles responded well on ovarian stimulation and went through ultrasound-guided follicular aspiration (UDFA).
The number of ova collected was 223, (an average of 11.73 ova per aspiration). They were checked for maturity and 196 (87.89%) of them were found to be at metaphase II stage which were selected for procedure ICSI/IVF/IVC. Twenty-seven (12.10%) ova were immature. Normal fertilisation rate (2PN) was achieved in 157 (80.10%) ova, whereas the overall fertilisation rate (1PN, 2PN, 3PN) was observed in 178 (90.81%) ova, (Table-2).
The embryo cleavage rate was 89.88% (n=160). Total 18 (94.7%) patients went through embryo transfer (ET) on day 2 or day 3. One patient developed ovarian hyperstimulation syndrome (OHSS) and her embryos remained vitrified. Clinical pregnancies were achieved in 03 patients and their embryos have remained vitrified for possible use in the future.
From the 125 vitrified embryos, 15 (12%) were warmed/thawed in order to perform transfer cycles in 04 (21.0%) patients. More than 50% of the blastomeres of 14 embryos were intact and all cells were viable at thawing, giving a survival rate of 93.33%.
After 24 hours of culture, almost all the embryos had divided, and the majority of the cleaved embryo had a quality score of Grade-I.
Discussion
It has been acknowledged without doubt that the routine use of a good, reliable and safe cryopreservation programme leads to improved cumulative clinical outcomes of IVF and ICSI cycles.9 The cost of a live birth could also be reduced by both preventing the repetitive use of expensive ovulation induction agents and avoiding the expensive clinical follow-up of ovulation induction cycles. However, the possibility of cell damage caused by cryopreservation is a major issue. Thus, several strategies to prevent cell damage have led to the introduction of different cryopreservation techniques over the past decades.10
The two most popular cryopreservation techniques of human embryos at different developmental stages are slow-rate freezing and vitrification. The slow-rate freeing method is also known as equilibrium freezing due to the exchange of fluids between the extra- and intra-cellular spaces.11 It was accepted to be a safe procedure because of the use of relatively low concentration of cryoprotectants that might not cause any serious toxic and osmotic damage. However, sub-zero temperatures and the conditions that the human oocytes and embryos are exposed to during cryopreservation are not physiological conditions.12 Therefore, these cells are susceptible to damage during all steps of cryopreservation procedures and the low concentrations of cryoprotectant are insufficient to avoid the formation of ice crystals, which is one of the main sources of cell injury. Also, previously reported low survival and pregnancy rates, along with the high cost of cryopreservation, has not satisfied the experts.13
In contrast, vitrification is a non-equilibrium method and may be regarded as a radical approach in which ice crystal formation is totally eliminated. Nevertheless, it requires an extremely high cooling rate alongside much higher concentration of cryoprotectants when compared with slow-rate freezing.9
In vitrification the problem of cytotoxicity has been overcome by using cryoprotectants with higher membrane permeability and lower toxicity, and possible use of combination with non-permeable cryoprotectants.14
In 1985, vitrification was reported for the first time as an efficient method in mouse embryo cryopreservation.15 Later, studies reported successful vitrification of human 4-8 cell embryos, and vitrification was suggested as a real alternative to slow-rate freezing.16
Thereafter, vitrification of human embryo, especially at early stages, became a more popular alternative due to comparable clinical and laboratory outcomes.17 Subsequently, available literature reported that survival rates following vitrification were positively correlated with the number of blastomeres in the cleavage-stage embryos.17 Survival rates of embryos were improved with the introduction of puncturing of the blastoceole prior to vitrification,18 and became superior to those obtained through slow-rate freezing.
Many variables in the vitrification process exist that can profoundly influence its effectiveness and the potential to improve the survival rates of the vitrified cells. These include (i) the type and concentration of cryoprotectant, (ii) the temperature of the vitrification solution at exposure, (iii) the duration of exposure to the final cryoprotectant before plunging into LN2 (liquid nitrogen), (iv) the type of device that is used for vitrification (which influences the size of the vapour coat and cooling rate), and (v) the quality and developmental stage of embryos. Increasing the speed of thermal conduction and decreasing the concentration of cryoprotectant is an ideal strategy for cryostorage of embryos with vitrification methods. However, the actual rate of heat transfer during vitrification procedures may vary extremely, depending on the device used, technical proficiency, and the specific movement at immersion.19
Subsequently, more encouraging survival rates have been reported for the vitrification of oocytes, cleavage stage embryos and zygotes and blastocyst stage embryos.20
In a randomised controlled clinical trial,4 241 embryos from 73 patients were vitrified and warmed, giving a clinical pregnancy rate of 49.3% and implantation rate of 29.7% of the vitrified embryo; which is the highest implantation and pregnancy rates following the vitrification technique.4
Another study21 compared the perinatal outcome of 413 cryoloop vitrified-warmed blastocyst transfers with that of 602 fresh blastocyst transfers. No significant differences were reported in the mean gestational age, birthweight, pre-term birth rate or congenital birth defect rate. Although this is encouraging, follow-up studies are necessary to ensure the safety of the technique. Global data support the hypothesis that vitrification is associated with less cellular trauma than slow-freezing and should be considered as the primary method of human embryo cryopreservation.4 Nowadays vitrification is claimed to be the future of cryopreservation of human embryos due to improved survival rate and pregnancy rate. The clinical application of this technology should ensure optimal survival of the embryos and oocytes that are stored and subsequently thawed for transfer. Vitrification is a promising technique in assisted reproductive technology, but comparative success rates are yet to be established.22
The current study relates to the first-year experience of cryopreservation through vitrification at SIRM. The fertilisation (80.10%) and cleavage (89.88%) rates achieved were quite promising for a new centre, when seen against the backdrop of 60-70% fertilization rate obtained with ICSI which was reported by pioneer researchers once the injection procedure had been optimised.23,24
Fifteen of the vitrified embryos were thawed in order to perform transfer cycles in 04 patients; the embryo survival rate was 93.33%. Multiple pregnancies are alarming, especially in parts of the world where neonatal care is scarce and expensive. The number of embryos transferred must be discussed with the couple and one must try to keep it at two only. The average number of ET per patient was 2.1 in this series. The pregnancy rate and taking-home-baby rates remain to be calculated by this relatively new technology.
Conclusion
Vitrification is a simple procedure that requires less time and is likely to become safer and were cost-effective with the passage of time. Survival rate of embryos is high, but actual efficacy needs to be studied further in Pakistani environment.
Acknowledgement
We are grateful to SIRM staff, especially Naheed Khan, Sajida Khan, Sabira Khan and Urooj Khan, for their assistance in various stages of data collection.
References
1. Kelly SM, Buckett WM, Abdul-Jalil AK, Tan SL. The cryobiology of assisted reproduction. Minerva Ginecol 2003; 55: 389-98.
2. Shaw JM, Jones GM. Terminology associated with vitrification and other cryopreservation procedures for oocytes and embryos. Hum Reprod Update 2003; 9: 583-605.
3. Anderson AR, Wilkinson SS, Price S, Crain JL. Reduction of high orders multiples in frozen embryos transfers. Reprod Biomed Online 2005; 10: 402-5.
4. Balaban B, Urman B, Ata B, Isiklar A, Larman MG, Hamilton R, et al. A randomized controlled study of human Day 3 embryo cryopreservation by slow freezing or vitrification: vitrification is associated with higher survival, metabolism and blastocyst formation. Hum Reprod 2008; 23: 1976-82.
5. Trounson A, Mohr L. Human pregnancy following cryopreservation, thawing and transfer of an eight- cell embryo. Nature1983; 305: 707-9.
6. Zeilmaker GH, Alberda AT, van Gent I, Rijkmans CM, Drogendijk AC. Two pregnancies following transfer of intact frozen-thawed embryos. Fertil Steril. 1984; 42: 293-6.
7. Kuwayama M, Vajta G, Kato O, Leibo SP. Highly efficient vitrification method for cryopreservation of human oocytes. Reprod Biomed Online. 2005; 11: 300-8.
8. Desai N, Blackmon H, Szeptycki J, Goldfarb J. Cryoloop vitrification of human day 3 cleavage-stage embryos: post-vitrification development, pregnancy outcomes and live births. Reprod Biomed Online 2007; 14: 208-13.
9. Vajta G, Nagy ZP. Are programmable freezers still needed in the embryo laboratory? Review on vitrification. Reprod Biomed Online 2006; 12: 779-96.
10. Vajta G, Holm P, Kuwayama M, Booth PJ, Jacobsen H, Greve T, et al. Open Pulled Straw (OPS) vitrification: a new way to reduce cryoinjuries of bovine ova and embryos. Mol Reprod Dev 1998; 51: 53-8.
11. Mazur P. Equilibrium, quasi- equilibrium and non equilibrium freezing of mammalian embryos. Cell Biophys 1990; 17: 53-92.
12. Menezo YJ, Nicollet B, Herbaut N, Andre D. Freezing cocultured human blastocysts. Fertil Steril 1992; 58: 977-80.
13. Fosas N, Marina F, Torres PJ, Jove I, Martin P, Perez N, et al. The births of five Spanish babies from cryopreserved donated oocytes. Hum Reprod 2003; 18: 1417-21.
14. Katayama KP, Stehlik J, Kuwayama M, Kato O, Stehlik E. High survival rate of vitrified human oocytes results in clinical pregnancy. Fertil Steril 2003; 80: 223-4.
15. Rall WF, Fahy GM. Ice-free cryopreservation of mouse embryos at -196 degree C by vitrification. Nature 1985; 313: 573-5.
16. Mukaida T, Wada S, Takahashi K Pedro PB, An TZ, Kasai M. Vitrification of human embryos based on the assessment of suitable conditions for 8-cell mouse embryos. Hum Reprod 1998; 13: 2874-9.
17. El-Danasouri I, Selman H. Successful pregnancies and deliveries after a simple vitrification protocol for day 3 human embryos. Fertil Steril 2001; 76: 400-2.
18. Vanderzwalman P, Bertin G, Debauche Ch, Standaert V, van Roosendaal E, Vandervorst M, et al. Births after vitrification at morula and blastocyst stages: effect of artificial reduction of the blastocoelic cavity before vitrification. Hum Reprod 2002; 17: 744-51.
19. Lane M, Gardner DK. Vitrification of mouse oocytes using a nylon loop. Mol Reprod Dev 2001; 58: 342-7.
20. Herdzak R, OstroA, Zdilov V, Toporcerová S, Kacmárik J. [Clinical experience with a modified method of human embryo vitrification]. Ceska Gynekol 2005; 70: 99-103.
21. Takahashi K, Mukaida T, Goto T, Oka C. Perinatal outcome of blastocyst transfer with vitrification using cryoloop: a 4-year follow-up study. Fertil Steril 2005; 84: 88-92.
22. Kuleshova LL, Lopata A. V itrification can be more favorable than slow cooling. Fertil Steril 2002; 78: 449-54.
23. Palermo G, Joris H, Derde MP, Camus M, Devroey P, Van Steirteghem A. Sperm characteristics and outcome of human assisted fertilization by subzonal insemination and intracytoplasmic sperm injection. Fertil Steril 1993; 59: 826-35.
24. Payne D, Flaherty SP, Jeffrey R, Warnes GM, Matthews CD. Successful treatment of severe male factor infertility in 100 consecutive cycles using intracytoplasmic sperm injection. Hum Reprod 1994; 9: 2051-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: