
N. Atiullah ( Department of Community Health Sciences, The Aga Khan University, Karachi. )
F.E Fikree ( Department of Community Health Sciences, The Aga Khan University, Karachi. )
I. Husain ( Department of Urological Surgery, Bedford Hospital, Bedford, England. )
February 1998, Volume 48, Issue 2
Original Article
Abstract
Cystitis is considered to be one of the most common infections afflicting women of all age groUps. It has been suggested that personal hygiene customs may influence the prevalence of cystitis. In this study, 130 women of child bearing age attending the out-patients clinic were interviewed in order to determine the frequency of cystitis and its associated risk factors including personal hygiene practices. Twenty seven percent of the women reported suffering from cystitis atleast once in the past, comparable to reported studies from the United States but higher than reported from other Muslim countries. Sixty-three percent of women reported their first episode during pregnancy and a significant relationship was observed between parity and cystitis (p value <0.000). However, personal hygiene practices following micturition or sexual intercourse bore no significant association with cystitis. Cystitis, commonly reported among Pakistani married women, occurs primarily during pregnancy. Preventive measures during pregnancy are suggested (JPMA 48:35.1998).
Introduction
Cystitis, an inflammation of the urinary bladder characterisedby symptoms of frequency and burning dysuria, is most commonly due to infection. Cystitis is considered by some physicians to be the most common bacterial infection in women1 and is second to common cold as a cause for out-patient visits. This is reflected in the high rates of cystitis: four out of five women in Britain will suffer the symptoms of cystitis at some time in their lives2. The vaginal reservoir and the short urethra in the female predispose to bacterial advancement resulting in much higher rates of cystitis among women than men. Predisposing risk factors include sexual activity3,4, use of diaphragm for contraception, catheterization5,6 and a past history of cystitis7. Personal hygiene customs have been shown to affect the prevalence of cystitis. It has been observed that careful washing with soap and water before and after sexual intercourse has proved most effective in reducing risk of re-infection in susceptible women8. On the other hand, a study to demonstrate a linkage between methods of wiping with toilet paper and the genesis of urinary tract infections was inconclusive due to difficulty in interpretation of responses from patients9. The use of toilet paper is virtually unknown in Muslim communities, where personal cleansing is effected exclusively with water10. It is feasible that this fact alone could simply account for the smaller number of women experiencing non-specific cystitis in these populations11. This paper reports on the frequency of cystitis among women from a facility-based population survey of an indigenous Muslim population in Karachi and examines the role playedby Islamic personal hygiene customs in the frequency of cystitis. This study is part of a multi-centered study which aims to relate differences in the frequency ofcystitis to variation in socio-cultural and personal hygiene practices among Islamic and non-Islamic communities in Norway, England, Saudi Arabia and Pakistan.
Materials and Methods
The study was carried out among women presenting to the consulting clinics of the Aga Khan University Hospital (AKUH), Karachi, during the period November 27 -December 1, 1994. Though AKUH is a private, tertiary care center, it caters to all socioeconomic strata of the city. Therefore, it may be assumed that a random selection of women attending the consulting clinics would be a true representationofthe female populationof Karachi. Pre-coded, close-ended, standard questionnaires were administered to 130 women in the child bearing age range (15-45 years) by a single interviewer, a physician. She randomly selected respondents from the pool of women in the waiting mom area and based on our selection criteria, proceeded to conduct the interviews. To eliminate selection bias, the eligibility criteria for selecting subjects was restricted to Muslim females who were accompanying patients to the clinics and were not patients themselves. The information obtained included past history of ever suffering fmm cystitis frequency, burning and dysuria], age, marital status, sexual activity, parity and personal hygiene habits related to micturition and sexual activity. To assess socio-econornic status, women were asked to report the gross monthly family income and the area of their residence. Different areas of the city were classified, according to standard norms, as high, upper middle, middle, lower middle and lower income group areas. There was a statistically significant correlation between reported household income and area of residence (p=0.000). The range in reported gross monthly family income and area of residence supported our assumption that AKUH caters to all socioeconomic strata of the city (Table I). The frequency of cystitis was defined as the percentage of women who ever reported suffering from cystitis while demographic and socio-cultural practices are those reported currently.
Discussion
A frequency of ever suffering from cystitis of 27% is reportedhere which suggeststhat almost three out of every ten women suffer from cystitis sometime during their life. Remis et al reports that an estimated 25-35% of women aged 20-40 years in the United States suffer atleast one episode of urinary tmct infection while a higher prevalence of four out of every five women is reported from Britain3. A frequency of 27% is comparable to reports from the United States but much lower than those from Great Britain3. However, reports from other muslim communities suggest that the frequency in this study is much higher11. One possible explanation of the higher frequency ofcystitis may be the high fertility rate of Pakistani Not only was a significant relationship between parity and cystitis observed but approximately two-thirds of the cystitis was reported as occuring during pregnancy. It is therefore suggested that preventive measures, such as careful washing with soap and water before and after sexual intercourse and after defecation, will reduce the risk of re-infection in susceptible pregnant women. In this study no association was found between personal cleansing hygiene following defecation or sexual activity and cystitis, though ever-married women are observed to be at significantly higher risk of suffering from cystitis as compared to single women (Table III). It appears that the lack of an association is primarily due to the majority of women following thà Islamic tradition of washing before and aftcr sexual intercourse as shown in Table I. The larger multi-centered study aimed to relate differences in the frequency of cystitis to variation in socio- cultural and personal hygiene practices among Islamic and non- Islamic communities in Norway, England. Saudi Arabia and Pakistan will demonstrate the association of the Islamic tradition of cleansing following defecation and prior and after sexual activity with cystilis.
Results
The mean age of the 130 women interviewed was 3 1±7.2 years. Of these, 28 (2 1.5%) were single and the remainder were currently either married (73.1%) or widowed/divorced (5.4%). The mean monthly income reported was Rs.8,900±7,003 (Table 1). Regarding socio-cultural practices among currently married women, 82% (78/95) reported frequency of sexual intercourse atleast once per week, 62% (59/95) washed both before and after sexual intercourse while only 24% (23/95) reported washing only after sexual intercourse (Table I).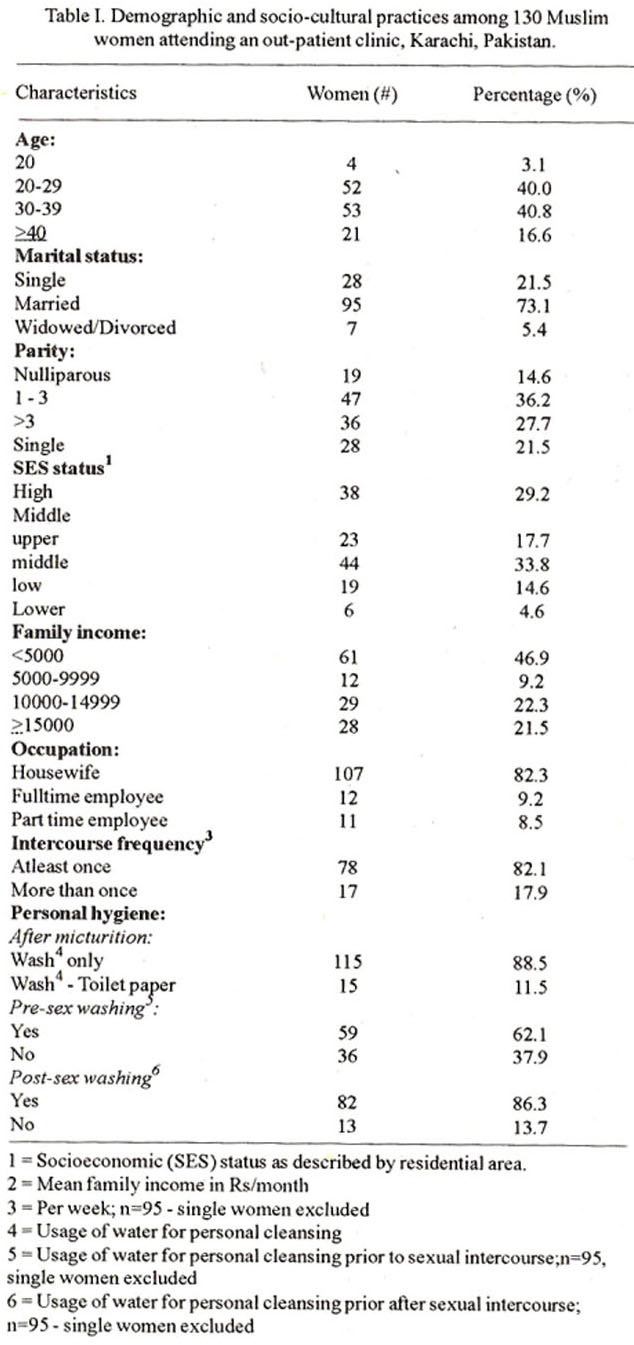
Thirty-five (26.9%) women reported suffering from cystitis atleast once in the past. Repeated episodes ofcystitis were reported by 40%(14/35) of cystitis sufferers. Twenty-two (63%) women bad their first episode during pregnancy while the remaining reported the first episode either during childhood (2/35=5.7%) or during their honeymoon (6/35=17%). Six (17%) of these 35 cystitis sufferers reported diabetes as a concurrent illness (Table II).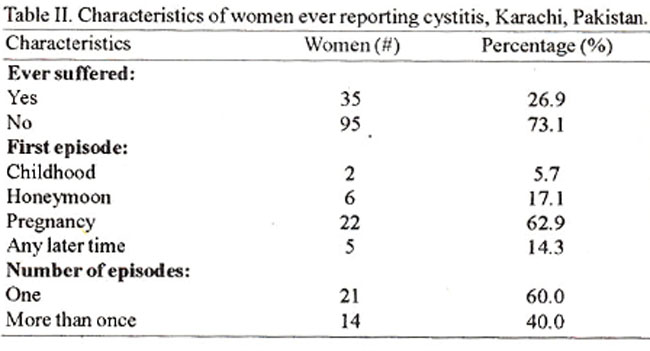
Ever-married women were at a significantly higher risk of developing cystitis as compared to single women. In addition, a significant linear trend was observed for parity with women mporting three or more live births at greatest risk ofcystitis as compared to single women. Women reporting an average monthly income of Rs.5,000 and over were at a significantly higher risk of cystitis as compared to lower income women. However, there was no significant association between cystitis and personal hygiene habits (Table III).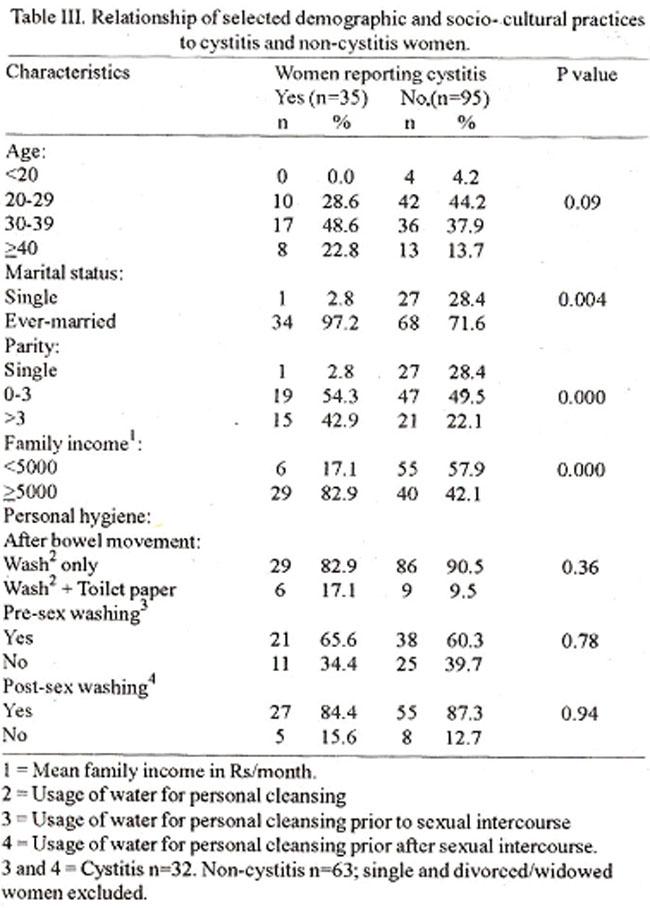
References
1. Tolkoff.Rubin, N.E. and Rubin, RH. New approaches to the treatment of UT!. Am. J.Med., 1987-82:270-277,
2. Williams, J. The burning issue. Cystitia update. Fam. Health, 1994;10:17-19.
3. Kunin, C.M and McCormack, R.C. An epidemiologic study ofbacteriuria and blood pressure among nuns and working women. N. Engl, J. Med., 1 968;278 :635-642.
4. Remia, R.S., Gurwith, M.J., Gurwith, D. et al. Risk factors for U.T.L .Am.J. Epidemiol., 1 987;126:685-689.
5. Kaye, M., de-Vriea, J. and Mac-Farlane, K.T. The initiation of U.T.L following a single bladder catheterization. Can. Med. Assoc. J., 1962;86 :9-12.
6. Theil, 0., Spuhler, 0. U.T.I. by catheter and the so called infectious (episomal) resistance. Schweiz. Med. Wochenachr., 1965;95: 1155-1163.
7. Kraft, J.K. and Stamey, T.A. The natural history of symptomatic recurrent bacteriuria in women. Medicine, 1977;56:55-60.
8. Kilmartin, A. Understanding cystitis. London, Arrow, 1992.
9. Marsh, PP., Murray, A., Panchamia, P. Therelationshipbetween bacterial cultures ofthevaginal introitua and urinary infection. Br. J. Urol., 1972;44:368-472.
10. Husain, 1. and Kazim, E. Urological evaluation of the tropical patient. In: Husain, I. (ed): Tropical Urology. Edinburgh and London, Churchill Livingstone, 1984, pp. 11-12.
11. Kazim, E., Ansari, E.M. and Husain,L The spectrum of genitourinasy disease seen in Abu Dhabi. Emirates Med. 3., 1981:2:76-83.
12. Pakistan Demographic and Health Survey 1990/91. National Institute of Population Studies, Islamabad. Pakistan and IRD. Calverton, MD, USA, Marco Intemational Inc., 1992.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: