
Aydin Unal ( Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
Mehmet Tugrul Inanc ( Department of Cardiology, Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
Nihat Kalay ( Department of Cardiology, Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
Ayse Ocak ( Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
Onur Kadir Uysal ( Department of Cardiology, Kayseri Education and Research Hospital, Erciyes University, Kayseri,Turkey. )
Abdurrahman Oguzhan ( Department of Cardiology, Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
Mustafa Duran ( Department of Cardiology, Kayseri Education and Research Hospital, Erciyes University, Kayseri,Turkey. )
Mehmet Gungor Kaya ( Department of Cardiology, Faculty of Medicine, Erciyes University, Kayseri,Turkey. )
June 2012, Volume 62, Issue 6
Original Article
Abstract
Objective: To evaluate the progression of carotid intima-media thickness (CIMT) and to search for possible associations between these changes and other risk factors of atherosclerosis for 2 years in stable patients with chronic renal failure (CRF) on haemodialysis (HD).
Methods: Study population consisted of 22 patients with newly diagnosed CRF. All patients underwent B-mode ultrasonography of common carotid artery for estimating CIMT and the presence of plaques before and after the first HD session (mean 24.22 ± 2.14 months). The differences in CIMT before and after long-term HD treatment were compared. Acute phase proteins, calcium-phosphate balance and lipid profile were assessed and anthropometric parameters were measured.
Results: Mean age was 55 ± 13 years and 10 (45%) of the patients were female. After long-term HD treatment, (mean 24.22 ± 2.14 months) the mean value for CIMT (0.57 ± 0.08 mm) was significantly lower than that at baseline (0.68 ± 0.12 mm) (p = 0.02). Only male gender and smoking were correlated with baseline CIMT. After long-term HD treatment, age, total cholesterol, LDL cholesterol, and triglyceride were related with CIMT. Diabetes and smoking were correlated with CIMT. Presence of plaque before HD only correlated with creatinine level and after long-term HD treatment only correlated with total cholesterol level.
Conclusion: We found that CIMT was significantly decreased 2 years after starting HD. An association between CIMT and other atherosclerotic risk factors (such as age, cholesterol, triglyceride etc.) could not be determined due to a small sample size.
Keywords: Chronic renal failure, Carotid artery intima-media thickness, Haemodialysis, Atherosclerosis, Ultrasonography (JPMA 62: 575; 2012).
Introduction
Cardiovascular disease is a main cause of morbidity and mortality in patients with chronic kidney disease (CKD), particularly those on dialysis.1,2 Atherosclerosis is the most frequent cause of cardiovascular morbidity in patients with CKD.3 An increased carotid intima-media thickness (CIMT) and the presence of plaques reflect generalized atherosclerosis. Therefore CIMT measurement has been proposed as a method for establishing risk stratification for cardiovascular events in both the general and the dialysis population.4,5 Measurement of CIMT with ultrasonography is a reliable, reproducible and non-invasive method for detecting the progression of atherosclerosis.4,5 In the present study, we aimed to evaluate the progression of CIMT and to search for possible associations between these changes and other risk factors of atherosclerosis on haemodialysis (HD) patients.
Patients and Methods
A prospective, non-randomized study was conducted on 50 patients, with newly diagnosed CKD and planned for HD treatment via an arteriovenous fistula (AVF). Eight of the 50 patients died during follow-up. Two patients underwent renal transplantation. Six patients refused control echocardiography. Twelve patients did not respond to our calls (lost to follow-up). Finally 22 patients were included in this study. We measured CIMT and assessed plaque occurrence in the carotid arteries by B-mode ultrasonography. After long term HD treatment (mean 24.22 ± 2.14 months) the second ultrasonographic evaluation was performed. The patients were given HD treatment three times a week for four hours. Clinical and laboratory data were obtained from the patients on the day of ultrasonographic examination at baseline and after 2 years. Systolic and diastolic blood pressures were routinely measured before and after haemodialysis. The local ethics committee approved the study, and informed consent was obtained from each patient.
Inclusion criteria were: newly diagnosed of ESRD, sinus rhythm, LV ejection fraction (EF) above 50%, no history of myocardial infarction, or evidence of valvular disease. Patients with cerebral vascular disease, clinical and electrocardiographic evidence of myocardial ischaemia, history of coronary artery disease, pericardial disease, heart failure (EF<50%), valvular heart disease and chronic pulmonary disease were excluded from the study.
Patients\\\' left and right common carotid arteries were examined ultrasonographically before creation of AVF and after long-term HD treatment. A high-resolution ultrasound system equipped with a 7-MHz linear transducer (Vivid 7 Dimension, General Electric Healthcare Company, Milwaukee, WI, USA) was used. All scans were performed by the same cardiologist (MD) who was blinded to the patients\\\' clinical and laboratory data. The CIMT was measured on the common carotid arteries bilaterally, 2-4 cm proximal to the bifurcations in the plaque-free section. Three digitalized still images from the same section of the artery were measured and the average value was calculated. For each subject, the mean CIMT was recorded as the average of the left and right CIMT. The difference in CIMT before and after HD was calculated (DCIMT) for all patients. The common, internal and external carotid arteries were also scanned longitudinally and transversely to assess occurrence of plaques before and after HD treatment.
SPSS 15.0 statistical software (SPSS, Chicago, IL, USA) was used for the statistical analysis. The Kolmogorov-Smirnov test was used to determine normality of distributions of variables. Continuous variables with normal distribution were presented as mean ± standard deviation. Median value was used in variables without normal distribution. The qualitative variables were expressed as percentages. To compare variables before and after HD treatment, paired t test (for parametric variables), Wilcoxon test (for the nonparametric variables), and McNemar test (for categorized variables) were used. The correlation analysis was evaluated by the Spearman\\\'s correlation test for all variables because the sample size was relatively small (< 30 patients). P value of <0.05 was considered to be significant.
Results
Demographic and clinical characteristics of the study population are shown in Table-1.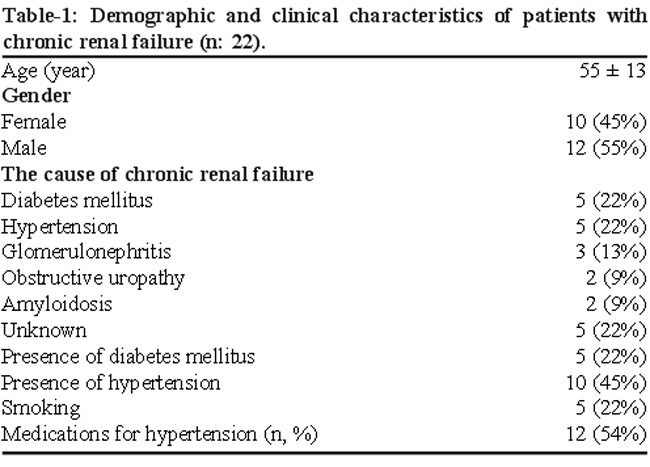
Mean age was 55 ± 13 years and 10 (45%) patients were female. The most common causes of CKD were diabetes mellitus and hypertension. Twelve patients with CKD were taking anti-hypertensive treatment before and after starting HD treatment. These anti-hypertensive agents were not modified or interrupted.
Comparison of biochemical and clinical findings before and after HD treatment are shown in Table 2.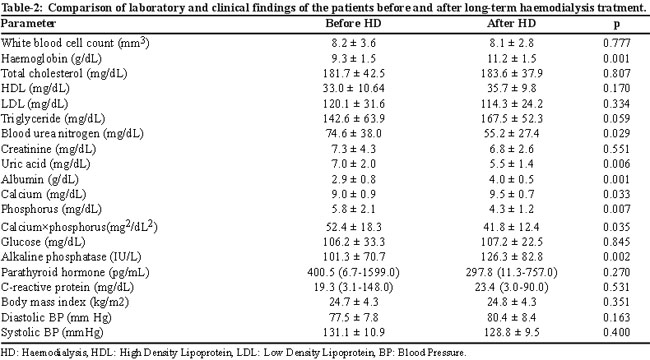
All variables tested as normally distributed except parathyroid hormone, C-reactive protein and CIMT after HD treatment. Levels of serum haemoglobin, albumin, calcium, and alkaline phosphatase were significantly increased after HD treatment compared to baseline values. In addition, levels of blood urea nitrogen, uric acid, phosphorus and calcium x phosphorus product were significantly decreased after HD treatment compared to baseline values. There was no significant difference regarding other parameters including white blood cell count, total cholesterol, high density lipoprotein, low density lipoprotein, triglyceride, serum creatinine, glucose, parathyroid hormone, C-reactive protein, body mass index, blood pressure between before and after HD treatment.
Before HD treatment, mean CIMT value was 0.62 ± 0.07 for women and 0.73 ± 0.13 for men. After long term HD, mean CIMT value was 0.55 ± 0.09 for women and 0.59 ± 0.07 for men. After long-term HD treatment, CIMT (0.57 ± 0.08) mm was significantly lower than that at baseline value (0.68 ± 0.12 mm) (p = 0.003). Five (22.7%) patients had carotid plaques in one or more sites.
Mean CIMT measured at baseline and after HD treatment were not significantly different between groups based on different causes of renal failure, and presence of hypertension and diabetes. The correlation between variables and CIMT before and after long-term HD treatment are shown in Table-3.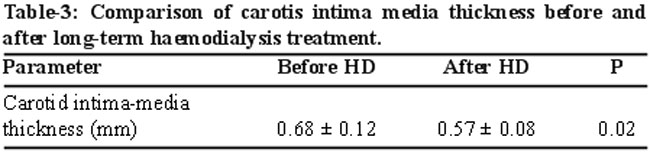
Only male gender and smoking were related with baseline CIMT. After long-term HD treatment, age, total cholesterol, LDL cholesterol, triglyceride and BMI were associated with CIMT. Diabetes, smoking and glucose level were correlated with DCIMT. Presence of plaque before HD only correlated with creatinine level and after long-term HD treatment only correlated with total cholesterol level.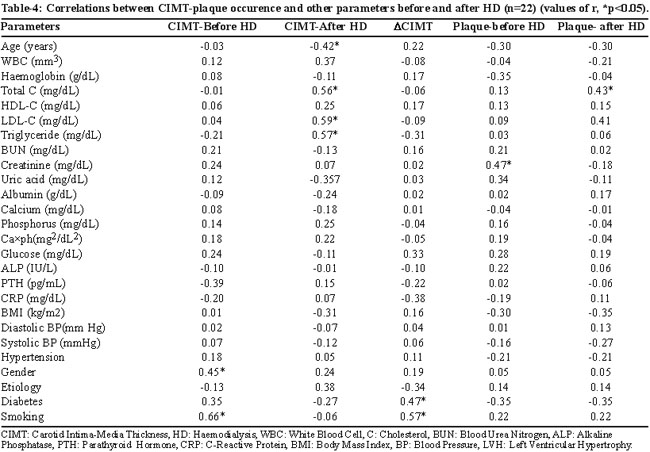
Discussion
The pathogenesis of cardiovascular damage in HD patients is complex. These patients were found to have traditional risk factors of advanced atherosclerosis as well as nontraditional factors that occur in patients with CKD.
In previous studies, a significant increase was found in CIMT and plaque occurrence in carotid arteries in HD patients compared to age- and sex-matched healthy control subjects.3,6 Also, a higher frequency of plaques in carotid arteries in HD patients was observed.3,6 Several studies have shown that CKD is one of the major contributor in the progression of atherosclerosis.1,7
Previous studies have demonstrated that the CIMT correlated significantly with age in patients with CKD.8,9 We found a significant negative association between CIMT and age after long-term HD treatment. This finding is consistent with reduction of CIMT in two years. Before starting HD treatment, neither CIMT nor plaque occurrence is associated with age. Kawagashi et al3 and London et al10 found an association between CIMT and smoking in HD patients. In the same line, we found positive association between smoking and basal CIMT and DCIMT. However, we did not observe an association between cigarette smoking and plaque occurrence.
Arterial hypertension is very common among patients with CKD. Previous studies did not confirm the role of blood pressure as a determinant of CIMT in HD patients.3,11 In our study, we also did not find an association between systolic and diastolic blood pressure, history of hypertension and CIMT, plaque occurence at basal and after HD treatment and DCIMT. These results can be explained by the fact that most hypertensive HD patients received long-term antihypertensive treatment and their blood pressure was well-controlled. Also their medical treatment may effect atherosclerosis in carotid artery.
Association of inflammatory markers and CIMT was shown in both the general and dialysis population.12,13 Okhuma et al found a significant correlation between CRP, serum calcium level and CIMT.14 In the same study they found a significant association between plaque score and CRP. High sensitivity CRP is also elevated in CKD and reflects micro and macroinflammation.15 Kawagashi et al. found a correlation between CIMT and serum phosphorus level and PTH in HD patients.3 Impaired calcium-phosphorus metabolism may affect lipoprotein metabolism and may contribute to the acceleration of atherosclerosis.3 Contrary to these findings, we found no correlation between CIMT and serum levels of calcium, phosphorus, calcium x phosporus product, PTH and CRP, which is compatible with some recent studies.10,16 Although we did not find a significant correlation between DCIMT and inflammation markers on univariate analysis, we observed a significant increase of haemoglobin, albumin, calcium and significant decreases of BUN, uric acid, phosphorus, calcium-phosphorus ion product which might contribute to decrease of CIMT in two years.
Association between CIMT and lipid disorders have inconsistently been reported in patients on dialysis.17 It has been demonstrated that an independent association exists between total cholesterol, LDL cholesterol, triglycerides and CIMT and plaque occurrence in HD patients.11,16,18 However, several studies reported no relationship between lipid profile and CIMT in HD patients.3,14,19 Although, the data are conflicting, our results support a relation between total cholesterol and CIMT and plaque occurrence after HD treatment. Also LDL cholesterol and triglyceride levels were associated with CIMT after HD treatment.
Albumin was also shown to be inversely and independently associated with CIMT in some studies of haemodialysis patients.10,20 Albumin may represent the state of enhanced inflammatory response as a negative acute-phase protein. However, we did not find an association between serum albumin and CIMT measured before and after HD treatment, DCIMT, plaque occurrence despite the fact that albumin concentration increased significantly during the 2 years follow-up.
Limitations of the study were that the sample size was relatively small (major limitation of our study) and lack of a control group. Secondly, we know that it is erroneous to perform a lot of univariate and regression analysis in only 22 patients but we performed this analysis to provide information on this topic. Thirdly, there may be many other variables such as influence of antihypertensive and antihyperlipidaemic medications, apolipoproteins and genetic markers that might have an impact on the progression of subclinical atherosclerosis, which we did not analyze in our study. Fourthly, we showed lipid profiles of patients and their changes with time but we did not have enough information on medication status of the patients (e.g. statins). Finally, the incidence of CKD in this region is not known.
Conclusion
To our knowledge this study has the longest follow-up period to provide data on the repeated measurement of CIMT. Contrary to previous studies, we found that CIMT was significantly decreased on HD patients in the long term. Although we found that decrease of CIMT might be due to decrease in BUN, uric acid, phosphorus, calcium-phosphorus ion product and increase in haemoglobin, albumin, and calcium, we must take into consideration that the sample size was too small to perform such an analysis.
References
1. Sarnak MJ, Levey AS. Epidemiology, diagnosis, and management of cardiac disease in chronic renal disease. J Thromb Thrombolysis 2000; 10:169-80.
2. Sit D, Kadiroglu AK, Kayabasi H, Kara IH, Yilmaz Z, Yilmaz ME. The evaluation incidence and risk factors of mortality among patients with end stage renal disease in southeast Turkey. Ren Fail 2008; 30: 37-44
3. Kawagishi T, Nishizawa Y, Konishi T, Kaivasaki K, Emoto M, Shoji T, et al. High-resolution B-mode ultrasonography in evaluation of atherosclerosis in uremia. Kidney Int 1995; 48: 820-6.
4. Lorenz MW, von Kegler S, Steinmetz H, Markus HS, Sitzer M. Carotid intima-media thickening indicates a higher vascular risk across a wide age range: Prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke 2006; 37: 87-92.
5. Nishizawa Y, Shoji T, Maekawa K, Nagasue K, Okuno S, Kim M, et al. Intima-media thickness of carotid artery predicts cardiovascular mortality in hemodialysis patients. Am J Kidney Dis 2003; 41: 76-9.
6. Hojs R. Carotid intima-media thickness and plaques in hemodialysis patients. Artif Organs 2000; 9: 691-5.
7. London G, Marchais S, Guerin A, Metivier F, Adda H. Arterial structure and function in end-stage renal disease. Nephrol Dial Transplant 2002; 17: 1713-24
8. Craven TE, Ryu JE, Espeland MA, Kahl FR, McKinney WM, Toole JF, et al. Evaluation of the association between carotid artery atherosclerosis and coronary artery stenosis: a case control study. Circulation 1990; 82: 1230-42.
9. Bevc S, Hojs R, Ekart R, Hojs-Fabjan T. Atherosclerosis in hemodialysis patients: traditional and nontraditional risk factors. Acta Dermatoven 2006; 15: 151-7.
10. Kato A, Takita T, Maruyama Y, Kumagai H, Hishida A. Impact of carotid atherosclerosis on long-term mortality in chronic hemodialysis patients. Kidney Int 2003; 64: 1472-9.
11. Burdick, L, Periti M, Salvaggio A, Bertolo S, Mangiarotti R, Castagnone D, et al. Relation between carotid artery atherosclerosis and time on dialysis. A non-invasive study. Clin Nephrol 1994; 42: 121-6.
12. Papagianni A, Kalovoulos M, Kirmizis D, Vainas A, Belechri AM, Alexopoulos E, et al. Carotid atherosclerosis is associated with in?ammation and endothelial cell adhesion molecules in chronic haemodialysis patients. Nephrol. Dial. Transplant 2003; 18: 113-9.
13. Zoccali C, Benedetto FA, Mallamaci F, Tripepi G, Fermo I, Foca A, et al. In?ammation is associated with carotid atherosclerosis in dialysis patients. Creed Investigators. Cardiovascular risk extended evaluation in dialysis patients. J Hypertens 2000; 18: 1207-13.
14. Okhuma T, Minagawa T, Takada N, Ohno M, Oda H,Ohashi H. C-reactive protein, lipoprotein (a), homocysteine, and male sex contribute to carotid atherosclerosis in peritonealdialysis patients. Am J Kidney Dis 2003; 42: 355-61.
15. Tsirpanlis G. In?ammation in atherosclerosis and other conditions: a response to danger. Kidney Blood Press Res 2005; 28: 211-7.
16. Hojs R, Hojs-Fabjan T, Pe~ovnik-Balon B. Atherosclerosis and risk factors in non-diabetic hemodialysis patients. Dial Transplant 2004; 10: 624-33.
17. Kalanthar-Zadeh K, Ikizler TA, Block G, Avram MM, Kopple JD. Malnutrition-in?ammation complex syndrome in dialysis patients: causes and consequences. Am J Kidney Dis 2003; 42: 864-81.
18. Drüeke T, Witko-Sarsat V, Massy Z, Descamps-Latscha B, Guerin AP, Marchais SJ, et al. Iron therapy, advanced oxidation protein products, and carotid artery intima-media thickness in end-stage renal disease. Circulation 2002; 106: 2212-7.
19. Oh J, Wunsch R, Turzer M, Bahner M, Raggi P, Querfeld U, et al. Advanced coronary and carotid arteriopathy in young adults with childhood-onset chronic renal failure. Circulation 2002; 106: 100-5.
20. Papagianni A, Kokolina E, Kalovoulos M, Vainas A, Dimitriadis C, Memmos D. Carotid atherosclerosis is associated with in?ammation, malnutrition and intercellular adhesion molecule-1 in patients on continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant 2004; 19: 1258-63.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: