
Yusuf Ustu ( Department of Family Medicine, Ankara Ataturk Training & Research Hospital, Ankara, Turkey. )
Mehmet Ugurlu ( Department of Family Medicine, Family Medicine Clinic of Samsun Training & Research Hospital, Samsun, Turkey. )
Ozlem Aslan ( Turkish Navy, Turkey. )
Yasar Metin Aksoy ( Department of Cardiothoracic Surgery, Tokat Training & Research Hospital, Tokat, Turkey. )
Ismail Kasim ( Department of Family Medicine, Family Medicine Clinic of Samsun Training & Research Hospital, Samsun, Turkey. )
Mehmet Taskin Egici ( Department of Family Medicine, Turkish Ministry of Health, Turkey. )
SelimYavuz Sanisoglu ( Department of Biostatistics, Turkish Ministry of Health, Turkey. )
May 2012, Volume 62, Issue 5
Original Article
Abstract
Objective: To determine the prevalence of overweight and obesity in the Tokat Region with demographic, socioeconomic and medical factors in the adult population.
Methods: A sample was selected from the province of Tokat. A total of 5162 participants over 18 years (1885 women and 3277 men) were included in the study. Demographic factors, family history of selected medical conditions, and lifestyle factors were obtained and blood pressure levels were measured for all participants. Obesity was defined as BMI > 30 kg/m2 and overweight as BMI between 25.0 to 29.9 kg/m2.
Results: The study demonstrated that the prevalence of overweight was 27.6% in men, 34.2% in women and 30% for overall. Obesity was prevalent in 33.6% men, 22.3% women, and 29.5% overall. The prevalence of obesity increased with age. Age, gender, educational level, marital status, hypertension, family histories of selected medical conditions were independently associated with obesity. Prevalence of hypertension increased with the degree of obesity. Results were in accordance with recent Turkish population-based obesity studies.
Conclusion: The data obtained showed that obesity prevalence was high in the study area. Primary prevention through lifestyle modifications may have a critical role in the control of obesity.
Keywords: Obesity, Body mass index, Hypertension, Associated risk factors, Turkish population, Tokat (JPMA 62: 435; 2012).
Introduction
Obesity is a major public health problem and the most common nutritional disorders.1 Overweight and obesity are associated with chronic diseases such as type 2 diabetes, hypertension, cardiovascular and cerebrovascular diseases, digestive disorders and cancer.2 Furthermore, obesity is a major independent risk factor in the development of hypertension.3 According to the World Health Organisation (WHO), the prevalence of obesity is increasing in developing countries as well as developed countries.4,5 The prevalence varies not only among regions and countries, but also among races and ethnic groups.3
We do not have enough data about the prevalence of obesity and associated risk factors in Turkey.6-8 This is the first research about obesity in Tokat province and its towns. Recent studies in Turkey have highlighted important regional differences not only in the prevalence of obesity, but also in the tendency for this prevalence to increase.9 Researches show that obesity prevalence increased between 1990 and 2000 (17.7%) in Turkey.10 The number of obese people increased in women 36%, and in men 75% during the last 10 years in Turkey.9,10 These results indicate the importance of monitoring obesity nationwide and in different regions of Turkey, because there is great difference in the socio-economical status among different parts of the country. In this cross-sectional study carried out in Tokat, the purpose was to find out the prevalence of obesity and to identify epidemiological risk factors.
Subjects and Methods
This cross-sectional descriptive study was undertaken in Tokat city and all its 11 towns, namely, Turhal, Yesilyurt, Zile, Resadiye, Almus, Basciftlik, Sulusaray, Artova, Erbaa, Niksar and Pazar, from January to June 2008. Situated in the northeastern part of Turkey, Tokat city has a population of 624,439. Random cluster sampling was applied to select the study subjects. Individuals over 18 years were selected from their family health cards. All the households were visited by field workers. Face-to-face interviews were arranged with 5661 subjects. As all inhabitants could not reach the interviewers, only 4817 people were included (2932 males and 1885 females). Demographic data were obtained for each subject. Measurements were made of weight (kg), height (m), BMI (weight/height2), waist and hip circumferences (cm), and the waist to hip ratio (WHR).11
Findings were classified as normal (18.50-24.9 kg/m2), overweight (25-29.9 kg/m2) and obesity (30-34.9 kg/m2). Underweight (<18.5 kg/m2) ones and pregnant were kept out of the study. Central obesity was defined as a waist circumference >88 cm in women and >102 cm in men.12
Systolic blood pressure (sBP) and diastolic blood pressure (dBP) were measured twice in the sitting position after a 15-min rest, and the mean was taken in all cases. Hypertension was defined as sBP > 140 mmHg, dBP > 90 mmHg, or the use of antihypertensive agents.
Demographic variables included age, gender, marital status, level of education, occupation and unemployment, chronic diseases and family history of obesity, diabetes and hypertension.
All statistical analyses were performed using SPSS version 15 (SPSS, Inc., Chicago, IL). Descriptive statistics for continuous and categorical variables were shown as the mean ± SD and percentages, respectively. Relations among the categorical variables were investigated with Chi-Square test. Student\\\'s t test was used to compare the means of two independent groups. The significance of unvaried differences was assessed with Student\\\'s t test. Multivariate logistic regression analysis with forward selection method also was performed to find the parameters effect on obesity (BMI > 30 kg/m2). For all statistical analyses, p value less than or equal to 0.01 was considered to be statistically significant.
Results
The average age of the 4817 people who participated in the study was 51.0±16.5 (men: 49.4 ± 16.5 and women: 53.8 ± 16.0). Of the population 2764 (56.6%) were living in the city center. There were 2764 (37.1%) women and 2764 (62.9%) men. Body Mass Index (BMI) was 27.8 ± 5.2 (men: 28.3 ± 5.7 and women: 27.0 ± 4.2) kg/m2).
When the participants were grouped by diseases, it was found that 2310 (47.95%) had hypertension, 574 (11.91%) had hyperlipidaemia, 470 (9.75%) had Diabetes Mellitus, 171 (3.55%) had Coronary Heart Disease and 957 (19.87%) had other chronic diseases.
Prevalence of obesity was in 1450 (30.1%) {men: 1030 (35.13%), women: 420 (22.28%)}. Prevalence of obesity was higher in men than in women (p < 0.0001). The prevalence of overweight was 644 (34.16%) in women and 790 (26.94%) in men. The combined prevalence of both overweight and obesity was 59.87%.
Highest obesity prevalence was in the 50-59 age group (42.1%) significantly higher than the other age groups (p<0.001) (Table-1).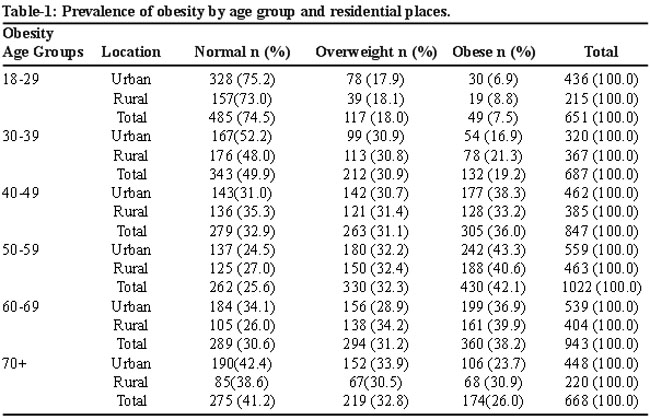
In all age groups, being overweight and obesity were increasing with age. This finding was supported by forward stepwise linear regression results in which addition of one unit age (year) had 0.387 kg/m2 and addition of one unit working duration (year) had 1.077 kg/m2 increase on BMI, respectively (Adj.R2= 0.932; F=22,418; p<0.001). It was also found that rural and urban life statistics were not significant (t=2.244; p=0.025). Besides mean obesity and overweight did not depend on the living place. Percentages of overweight and obesity in 20-60 age groups by decades were 25.3%, 50.1%, 67.1% and 74.4%; overall percentage being 59.87%.
In the urban area, obesity ratio of females (55.9%) was significantly higher than males (44.45%) (c2=27.499; p<0.001). The same results were found for the rural area, where, obesity ratio for women and men were 59.8% and 47.6%, respectively (c2=21.886; p<0.001).
Obesity rates were increasing with age in both women and men. This increase in women was steady, but in men it showed some spikes. In the 30-39 age group in men, overweight and obesity was almost double according to previous age group (53.1% in 30-39 to 25.3% in 20-29 age group).
Obesity was increasing with age and it reached the highest level for the 50-59 and 60-69 age groups. Especially in the 50+ age group, obesity in women was higher than in men. Evaluating age groups, there was another flashing finding that, in men, obesity was 11.8% in — the under 29 age group, but after 30, it had a very high increase (p < 0.0001; Table-2).
According to waist girth (n=2002), prevalence of central obesity was 617 (32.73%) in women; 1385 (47.23%) in men (p<0,0001). Prevalence of central obesity based on waist girth was comparable with that of general obesity defined by BMI. Prevalence of central obesity was high in both genders.
The prevalence of hypertension was 1226 (41.8%) among men, and 723 (38.3%) among women (p = 0.031). Total prevalence of hypertension was 40.5%.
There was a strong linear association between BMI and hypertension (p < 0.0001; Table-3).
The prevalence of hypertension was 48.8 % in obese subjects. Obesity and hypertension was positively and strongly correlated especially in women than in men (p<0.001).
In order to investigate the parametres had significant effect on obesity, multivariate logistics regression analysis was applied. The results showed that obesity probability of males was 1.936 times, and hypertension probability was 1.364 times higher than the females. Another significant parametre was age. It was also found that one-unit increase in the age affected the probability of obesity with the factor of 0.994 (c2= 62.290; p<0.001).
When considering the marital status and education levels, it was found that 50% of the married ones had obesity (40.2% in females and 56.3% in males). However, the ratio was getting smaller i.e. 36.5% for singles (17.9% for females and 51.4% for the males). It was also found that the obesity level was decreasing with increase in the level of education (c2=60.126; p<0.001). The obesity among the illiterate people was 60.5% (56.3% for females and 60.5% for males) and amongst university or higher degree holders it was as low as 28.7% (30.0% for females and 25.0% for males). However, some parametres such as living alone, occupation and unemployment were found to be insignificant. The prevalence of obesity in persons who had a family history of obesity, hypertension or diabetes was higher than in the persons who had no family history (p<0.0001).
Discussion
Obesity is one of the most important social and health problems in developed and developing countries.13 It is an important risk factor for other diseases and its prevalence is increasing worldwide (varies from 2% to 80%), including Turkey.14,15
The present study is a population-based survey of obesity in which the prevalence of overweight and obesity and associated risk factors were analysed for the first time in the Tokat region of Turkey.
Of the study populations, 56.6% were living in urban areas which is very close to Tokat\\\'s urbanisation ratio of 56.1%.16 This was considered to be a confidence increasing point on the reliability of the study results.
In our study, the prevalence of overall obesity was 29.5%. The combined prevalence of both overweight and obesity was high (59.5%). The prevalence of central obesity was 57.6% among women and 45.67% among men. These values were higher than the prevalence of overall obesity. An interesting finding was the relatively high ratio of obesity in men (33.6%) than women (22.3%). And overweight prevalence was higher in women (34.2%) compared to men (22.3%). Three major studies — TEKHARF (Turkish Adults Heart Disease and Risk Factors Study) in 1990, TURDEP (Turkish Diabetes Epidemiology Study) in 1999 and TOHS (The Turkish Obesity and Hypertension Study) in 2000 — studied obesity. In TURDEP study (24788 persons data utilised), the obesity prevalence (BMI>29.9 kg/m2) was found to be 22,3%17 (the prevalence rate in women (29.9%) was higher than in men (12.9%) (p < 0.001)), while in TEKHARF study (3687 persons data utilised) it was found to be 18.6% (12.5% among males and 32% in females). In TOHS study (23.888 persons data utilised), the obesity prevalence (BMI>29.9 kg/m2) was found to be 19.4% (14.4% among males, 24.6% in females). Recent local field studies in Adana (Prevalence of obesity: 43.4%),18 Trabzon (19.2%), Edirne (27.3%), Mersin (29.3%),19 Kayseri (12%),20 and Konya (23.7%),21 have revealed the current magnitude of obesity in Turkey. Delibasi et al9 study revealed obesity (8.674 persons data utilised) (17.4% in men and 20.4% in women) in the year 1999-2000. Recent studies (covering 15,468 people) for Turkey in general and detailed study utilising IDF (International Diabetes Federation) definition revealed the fact that female obesity percentage was 41.3% and male obesity was 21.2%.22 The prevalence of persons with a BMI > 30 kg/m2 (29,5%) was higher than in most other studies on obesity in Turkey,7,8,17,19-21 in which the prevalence varied from 12% to 29.3%. In the TEKHARF study, the prevalence of obesity was 32.1% in adults over 18 years of age. Another study in Adana (south of Turkey) confirmed a higher prevalence of obesity (43.4%). These prevalence are all much higher than previously reported.
Age was strongly associated with obesity. In many studies, it has been reported that prevalence of obesity increases with age.9,23-25 In our study, prevalence increased with age for both women and men. Especially in the 50+ age group, obesity in women was higher than in men. The highest prevalence of obesity was in the 50-to-59 age group for both women (29.1%) and men (50.6%). These results were similar to previous studies in Turkey.7,9,17-19 This association between obesity and age can be explained, in part, by a decrease in the degree of physical activity with age in both men and women.9,26 This increase in BMI warns us of the existence of dynamic process of weight-gain. Reduced physical activity is the main cause of the current epidemic of obesity in developed countries.27 A self-reporting study in 1999 reported that obesity prevalence was about 10% and overweight prevalence was 36.6% and 25.6% among males and females in 15 European Union countries. Also in different studies around the world, whether designed along regional or national lines, the obesity prevalence has been found to be ranging between 1% and 59% which overweight prevalence has been found ranging between 4% and 34% in different countries.28 Obesity rates in South and East Asian men and women are less than 7%. But this rate is more than 36% for both sexes in Canada and 38-40% in the Middle East and North and South Africa.29 Compared with other surveys in Europea (Britain), America, Australia, Middle East, Asia (Israel, Kuwait and Bahrain), Latin America (Uruguay), the prevalence of obesity in Tokat is lower than in Kuwait (30.3%), Bahrain (44%) and US (30.5%),30 but higher than Britain (19%) and Australia (20.8%).31
In the available literature, obesity is more prevalent among women than among men.32,33 The variation may be explained by differential distribution in risk factors (e.g., genetic predisposition, dietary factors, lack of physical activity) between women and men across populations.
Moreover, differences in prevalence of overweight and obesity in men among the different towns may be explained by men\\\'s more sedentary lifestyle and custom of sitting for long hours in some cafe.
Women were also prone to weight-gain during menopause. The loss of the menstrual cycle affects calorie intake and slightly lowers metabolic consumption, although most weight-gain has been attributed to a reduction in physical activity.4 Some studies reported that prevalence of obesity was higher in urban areas than in rural areas.34 Interestingly, in contrast to previous studies we could not find a statistically significant difference between the two sets of population. This may be explained by rapid migration towards urban areas from rural areas. This may also be a result of the similar lifestyles of urban and rural areas.
The risk of being obese was greater in persons with no formal education.35 In our study, obesity had a correlation with the level of education. Our study found that the higher the education level, the lower the obesity. The highest prevalence of obesity was in illiterate people (39.1%). Education (physically active, lifestyle and promoting nutritional awareness) can be effective for preventing obesity. The results were in line with studies conducted in Turkey and Europe.7-9,36,37
The relationship between marital status and prevalence of obesity is poorly defined, but studies have generally found that married men, though not always, weigh more than unmarried persons.38
Laurier et al., in a comparative survey in France, the United Kingdom, and the United States, have reported that married men or those living as part of a couple are twice as likely to be obese than those living alone.39 Our findings confirmed the literature (prevalence of obesity was 38.8% in widowed people and 31.0% in married people and 7.5% in unmarried people). Other researchers using multivariate analysis have reported that the prevalence of obesity in widowed people was higher than that in single and married subjects.40
Subjects with a family history of obesity, diabetes and hypertension have a greater prevalence of obesity compared with those without a family history.41 Our data showed that the prevalence of obesity was significantly higher in subjects with a family history.
Obesity has been observed to be a prime risk factor for the development of hypertension.42 Our data showed that blood pressure increased with the degree of obesity (p<0.0001). A previous community-based survey found that obesity was more prevalent in hypertensive subjects.6,7,9,43,44 Each unit of BMI increase causing 0.5 - 1.0 mm Hg increase in systolic blood pressure was related to obesity and hypertension risk.45,46 In our study, it was found that obese and high-weight groups had higher frequency of hypertension and it was statistically meaningful (p<0.001).
Such a difference in Turkey and developing countries might be due to socio-cultural factors, nourishment habits and also smoking among men and lack of employment outside the home among women.
Conclusion
The study showed that the prevalence of obesity in adults in Tokat city in Turkey was high. Prevalence of obesity has been increasing for Tokat, Turkey, and throughout the world. The most important consequence of the study was that almost all the factors were potentially modifiable and preventable. There is a need for an effective public health programme and urgent precautions for the control of obesity. The outcome of prevention and treatment should be evaluated by periodic national comparative surveys with standardised methods that would give us the actual trend.
Reference
1. Yanowski SZ, Yanowski JA. Obesity. N Engl J Med 2002; 346: 591-602.
2. Björntorp P. The association between obesity, adipose tissue distribution and disease. Acta Med Scand 1988; 723(suppl): 121-34.
3. Jia WP, Xiang KS, Chen L, Lu JX, Wu YM. Epidemiological study on obesity and its comorbidities in urban Chinese older than 20 years of age in Shanghai, China. Obes Rev 2002; 3: 57-65.
4. World Health Organization : Obesity: Preventing and managing the global epidemic. Report of a WHO Consultation on obesity. Geneva, Switzerland: WHO, 1998.
5. World Health Organization. Controlling The Global Obesity Epidemic. WHO, 2001.
6. Onat A, Sansoy V, Ökçün B, Kahraman G, Dursunoglu D. Türk Eriskinlerinde Glukoz intoleransi ve Diyabeti Türk Eriskinlerinde Kalp Saglinin Dünü ve Bugünü (TEKHARF Çalismasi). Istanbul: Karakter Color Basimevi, 1996; pp 103-11.
7. Erem C, Yildiz R, Kavgaci H, Karahan C, Deger O, Can G, et al. Prevalence of diabetes, obesity and hypertension in a Turkish population (Trabzon city). Diabetes Res Clin Prac 2001; 54: 203-8.
8. Hatemi H, Turan N, Arik N, Yumuk V. The Türkish Obesity and hypertension Study (TOHS). Endokrinolojide Yönelisler Dergisi, 2002; 11 (1).
9. T Delibasu Y. Karaaslan I. Üstün E. Köroglu S. Hosgör. National prevalence of underweight, overweight and obesity in Turkey: cross sectional study of a representative adult population. Cent Europ J Med 2007; 2: 294-303.
10. Yumuk VD. Prevalence of obesity in Turkey. Obes Rev 2005; 6: pp 9-10.
11. WHO MONICA Project: Population survey data compenent. In: MON?CA Manual. Geneva, Switzerland; WHO 1990; part III, section 1.
12. Expert Panel on Detection, Evaluatgion and Treatment of High Blood Cholesterol in Adults. Executive Summaryof the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
13. Deppeuch F,Maire B. Obesity and developing countries of the South. Med trop (Mars) 1997; 57: 380-8.
14. Gutierrez-Fisac JL, Banegus JR, Rodriguez Artalejo F, Regidor E. Increasing prevalence of overweight an obesity among Spanish adults, 1987-1997. Int J Obes 2000; 24: 1677-82.
15. The DECODA Study Group; European Diabetes Epidemiology Group. Age, body mass index and glucose tolerance in 11 European population-based surveys. Diabet med 2002; 19: 558-67.
16. (Online) (Cited 2011 Feb 10). Available from URL: http://tuikapp.tuik.gov.tr/adnksdagitapp/adnks.zul.
17. Satman I, Yilmaz MT, Sengül A, Salman S, Salman F, Uygur S, et al. The Turdep Group: Population-based study of diabetes and risk characteristics in Turkey: results of Türkisch Diabetes Epidemiology Study. Diabetes Care 2002; 25: 1551-6.
18. Gökçel A, Özsahin AK, Sezgin N, Karaköse H, Ertörer ME, Akbaba M, et al. High prevalence of diabetes in Adana, a southern province of Turkey. Diabetes Care 2003; 26: 3031-4.
19. Akbay E, Bugdayci R, Tezcan H, Konca K, Yazar A, Pata C. The prevalence of obesity in adult population in a city on the Mediterranean coast of Turkey. Türk J Endocrinol Metab 2003; 7: 31-5.
20. Kelestimur F, Cetin M, Pasaoglu H, Çoksevim B, Çetinkaya F, Ünlühizarci K, et al. The prevalence and identification of risk factors for type 2 diabetes mellitus and impairede glucose tolerance in Kayseri, central Anatolia, Turkey, Acta Diabetol 1999; 36: 85-91.
21. Yumuk VD, Hatemi H, Tarkci T, Uyar N, Turan N, et al. High prevalence of obesity and diabetes mellitus in Konya, a cental Anatolian city in Turkey). Diabetes Res Clin Prac 2005; 70: 151-8.
22. Sanisoglu SY, Oktenli C, Hasimi A, Yokusoglu M, Ugurlu M. Metabolic Syndrome Related Disorders in a large population of Turkey, BMC Public Health 2006; 6: 92.
23. Stene LC M, Giacaman R, Abdul-Rahim H, Husseini A, Norum KR, Holmboe-Ottesen G. Obesity and associated factors in a Palestinian West Bank village population. Eur J Clin Nutr 2001; 55: 805-11.
24. Martinez-Ros MT, Tormo MJ, Navarro C, Chirlaque MD, Perez-Flores D. Extremely high prevalence of overweight and obesity in Murcia, a Mediterranean region in sauth-east Spain. Int J Obes 2001; 25: 1372-80.
25. Fanghanel G, Sanchez-Reyes L, Berber A, Gomez-Santos R. Evaluation of the prevalence of obesity in the workers of a general hospital in Mexico. Obes Res 2001; 9: 268-73.
26. Gutierrez-Fisac JL, Regidor E, Rodriguez C. Economic and social factors associated with body mass index and obesity in the Spanish population aged 20-64 y. Eur J Public Health 1995; 5: 193-8.
27. Prentice AM, Jebb SA. Obesity in Britain: Gluttony or Stoth, Br med J 1995; 311: 437-9.
28. Martinez JA, Kearney JM, Kafatos A, Paguet S, Martinez-Gonzales MA. Variables independently associated with self-reported obesity in European Union. Public Health Nutr 1999; 2: 125-33.
29. Balkau B, Deanfield JE, Despres JP, Bassand JP, Fox KA, Smitth Jr SC, et al. International Day for the Evaluation of Abdominal Obesity (IDEA): a study of waist circumference, cardiovascular disease, and diabetes mellitus in 168.000 primary care patients in 63 countries. Circulation 2007; 116: 1942-51.
30. Flegal KM, Carroll MD, Ogden CL, Jahnson CL.Prevalence and trends in obesity among US adults. 1999-2000. JAMA 2002; 288: 1723-7.
31. Cameron AJ, Welbourn TA, Zimmet PZ, Dunstan DW, Owen N, Salmon J, et al. Overweight and obesity in Australia: the 1999-2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Med J Aus 2003; 178: 427-32.
32. Musaiger AO, Al-Mannai MA. Weight, height, body mass index and prevalence of obesity among the adult population in Bahrain. Ann Hum Biol 2001; 28: 346-50.
33. Alsaif MA, Hakim IA, Harris RB, Alduwahy M, Al Rabeaari K, Al Nuaim AR, et al. Prevalence and risk factors of obesity and overweight in adult Saudi population. Nutr Res 2002; 22: 1243-52.
34. Rashidi A, Mohammadpour-Ahranjani B, Vafa MR, Karandish M. "Prevalence of obesity in Iran." Obes Rev 2000; 6: 187-9.
35. Sobal J, Stunkard AJ. Socioeconomic status and obesity: A review of the literature. Psychol Bull 1989; 105: 260-75.
36. Stam-Moraga MC, Kolanowski J, Dramaix M, Henauw SD, De Bacquer DG, Kornitzer MD. Trends in the prevalence of obesity among Belgian men at work, 1977-1992. Int J Obes 1998; 22: 988-92.
37. Quiles Izquierdo J, Vioque J. Prevalencia de obesidad en la Comunidad Valenciana. Med Clin 1996; 106: 529-33.
38. Sobal J, Rauschembach B, Frongilio E. Marital status, fatness and obesity. Soc Sci Med 1992; 35: 915-23.
39. Laurier D, Guiguet M, Chau NP, Wells JA, Valleron AJ. Prevalence of obesity: a comparative survey in France, the United Kingdom and the United States. Int J Obes 1992; 16: 565-72.
40. Al-Mannai A, Dickerson JW, Morgan JB, Khalfan H. Obesity in Bahraini adults. J R Soc Health 1996; 116: 30-2.
41. Dhurandhar NV, Kulkarni PR. Prevalence of obesity in Bombay. Int J Obes Relat Metab Disord 1992; 16: 367-75.
42. Kunz I, Schorr U, Klaus S, Sharma AM. Resting metabolic rate and substrate use in obesity hypertension. Hypertension 2000; 36: 26-32.
43. Brown CD, Higgins M, Donato KA, Rohde FC, Garrison R, Obarzanek E, et al. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res 2000; 8: 676-7.
44. Stamler R, Stamler J, Riedlinger WF, Algera G, Roberts RH. Weight and blood pressure. Findings in hypertension screening of 1 million Americans. JAMA 1978; 240: 1607-10.
45. Brown CD, Higgins M Donato KA ve ark. Body mass index and the prevalence of hypertension and dislipidemia. Obes Res 2000; 8: 605-19.
46. Ghannem H, Fredj AH. Prevalence of cardiovascular risk factors in the urban population of Soussa in Tunisia. J Public Health Med 1997; 19: 392-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: