
Samina Ismail ( Department of Anaesthesia, Aga Khan University Hospital, Karachi. )
Faraz Shafiq ( Department of Anaesthesia, Aga Khan University Hospital, Karachi. )
Aliya Malik ( Department of Anaesthesia, Aga Khan University Hospital, Karachi. )
April 2012, Volume 62, Issue 4
Original Article
Abstract
Objective: The percentage use of regional anaesthesia (RA) and failure rate of RA for different grades of caesarean section (CS) has become a marker of quality for obstetric anaesthesia service. The objective of our prospective observational study is to find out the technique of anaesthesia used in different grades of CS, reasons for choosing general anaesthesia (GA) and failure rate of RA in our hospital setting.
Methods: This prospective cross sectional study was carried in the obstetric unit of Aga Khan University Hospital from 1st January 2010 to 31st May 2011. The anaesthetist performing the procedure filled out the data collection proforma .Suggested Indicators were percentages of Grade 1-4 CS done under RA and GA, percent of failed regional, percent of failed regional in different grades of CS.
Results: A total of 407 patients having undergone Caesarian Section (CS) were reviewed. General Anaesthesia (GA) was used in 201(49%) patients and Regional Anaesthesia (RA) in 206 (51%) patients. There was no significant difference between the use of GA and RA for grade 2-4 CS {grade 2: GA 42 (51%), RA 40 (49%), grade 3: GA 43 (46%), RA 39 (53%), grade 4: GA 81 (44%), RA 101 (55%) with a slight increase margin of difference for grade1 CS {GA 44 (63%) vs RA 26 (37%)}.
Patient preference 42 (45%)was the most common reason for choosing General Anaesthesia.. Fourteen (6.7%) patients required conversion from regional technique to GA. Of these 11 patients had Grade 1-3 CS and three patients had grade 4 or elective CS.
Conclusion: A large percentage (49%) of patients preferred general anaesthesia for CS which is of the International standards. This calls for guidelines regarding the use of Regional Anaesthesia for different grades Caesarian Section. Patient education regarding the use and benefits of Regional Anaesthesia needs to enforced.
Keywords: Caesarian section, General anaesthesia, Regional anaesthesia (JPMA 62: 363; 2012).
Introduction
Regional anaesthesia (RA) for caesarean section (CS) is the preferred option when calculating the risks and benefits for the mother and the foetus. The Royal College of Anaesthetists audit guidelines suggest that 85% of emergency CS should be conducted under RA, and the conversion to general anaesthesia (GA) should be less than 3% for emergency, and less than 1% for elective surgery.1
The percentage use of RA for CS has become a marker of quality for obstetric anaesthesia service.11 Similarly, factors like failure of RA and urgency of CS have also become the main quality indicators. The urgency of CS is classified into four grades by Lucas et al2 and is recommended by the National Institute for Clinical Excellence (NICE) in 2004.3 According to this classification, emergency and elective caesarean section equate to categories 1-3, and category 4 respectively.
In our setup, there is no standard protocol for the selection of RA in CS patients. Most patients prefer GA, because of poor counselling and myths related to the RA. The issue becomes more important when we talk about Grade 1 CS, where most surgeons prefer the provision of GA. The common causes of this behaviour are traditional beliefs like delay in readiness of the patient for surgery and the fear of failure of adequate block for the surgery.
The objective of our prospective observational study was to find out the technique of anaesthesia used in different grades of CS, reasons for choosing GA, and the failure rate of RA in our hospital setting. Our study further aimed at evaluating the level of supervision and choice of anaesthesia for different work hours.
Subjects and Methods
The prospective cross-sectional study was carried in the obstetric unit of Aga Khan University Hospital. After taking approval from the hospital\\\'s ethics committee, all caesarean sections done from January to May 2010 were included. The anaesthetist performing the procedure filled out the data-collection proforma after consultation with the obstetrician. The data included the technique of anaesthesia chosen by the anaesthetist, reason for choosing GA, level of supervision and urgency of delivery classified using the four-grade scale. If a regional technique failed, its details were noted down. This included possible reason of failure; whether the anaesthetist was unable to institute the regional technique or it failed to work after institution, what was the level of anaesthetist performing the procedure, what was the level of supervision and timings of work hours. Patients\\\' hospital number was noted to get any missing information. The proforma were collected and reviewed by one of the investigators for any missing data on a daily basis.
Suggested Indicators were percentages of grade 1-4 CS done under RA and GA, overall percentage of failed RA, and percentage of failed RA in different grades of CS.
The Statistical Package of Social Sciences (SPSS) version 17 was used for data entry and analysis. Multiple bar charts for type of anaesthesia technique with grade of CS, and the level of supervision with the duty hours were generated. The rest of variables, including the anaesthesia technique of choice, reasons for choosing GA, level of supervision and the reasons for the failure of RA, were analysed by generating frequencies and percentages.
Results
A total of 407 patients having caesarean deliveries during the study period were received. According to Lucas2 CS classification, 69 (17%) patients had Grade 1 CS, 82 (20%) patients had Grade 2, 73 (18%) patients had Grade 3, while 183 (45%) patients had Grade 4 CS indication.
In 201 (49%) patients, GA was the technique of choice, whereas RA was selected in 206 (51%) patients. Among patients who were given RA, 181 (87.5%) had spinal anaesthesia, 24 (12.0%) had extension of labour epidural analgesia, and 1 (0.5%) parturient had combined spinal epidural anaesthesia.
The use of general and regional anaesthesia for different grades of CS (Figure-1)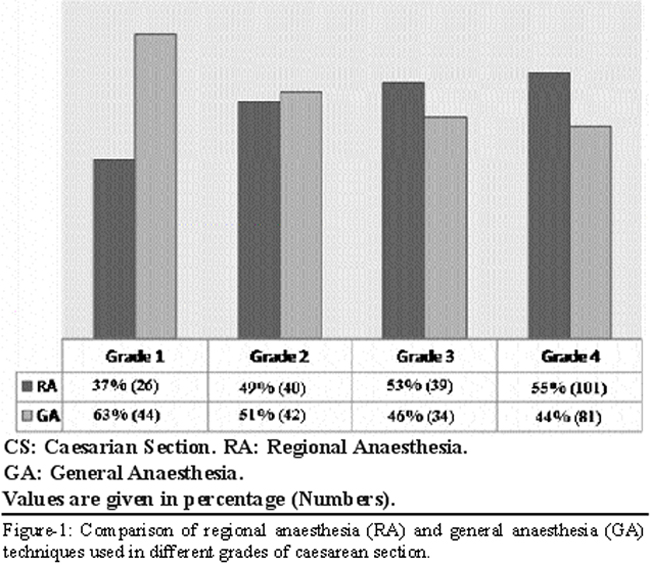
showed a high rate (44%) of elective CS done under GA. The same trend of high percentage of GA for Grade 4 CS was shown by our retrospective analysis from 2007-2009 (Figure-2).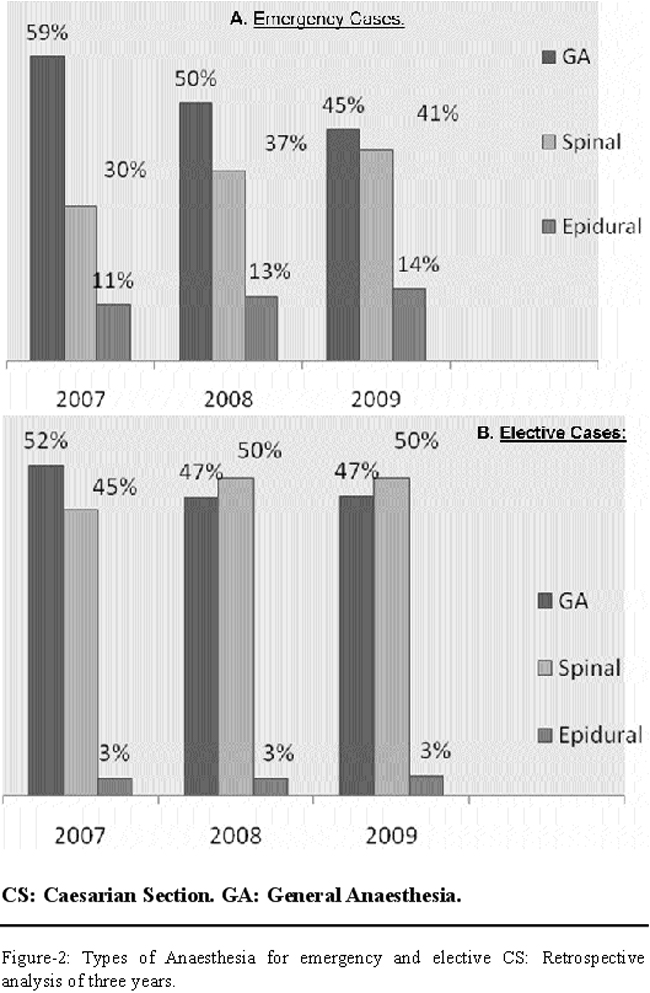
On evaluating the reason for choosing GA, patients\\\' refusal 91 (45%) cases was the most common factor, followed by anaesthetist choice in 35 ((17%) patients, surgeon\\\'s choice in 20 (10%) patients, lack of time in 35 (17%) patients and miscellaneous causes in 18 (9%).
Evaluation of the effect of work hours and level of supervision on the choice of anaesthesia showed that 286 (70%) surgeries were done during the morning shift (8.00-1700 hours), 59 (14%) surgeries were done in the evening shift (17.00-20.30 hours), while 62 (15%) surgeries were performed during the on-call hours (20.30-8.00 hours). The technique of anaesthesia chosen did not show any change for different work hours. The level of supervision changed with different work hours (Figure-3)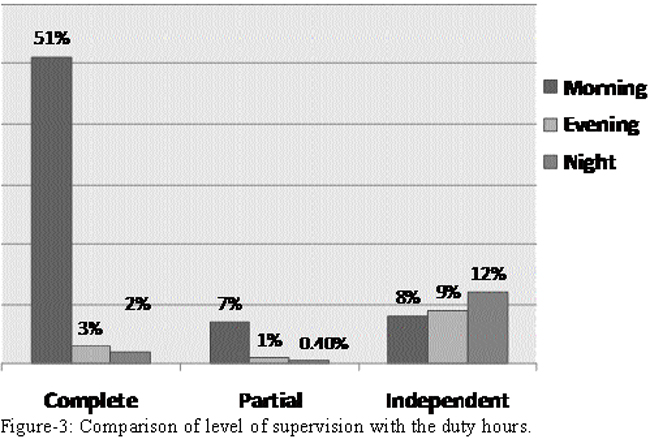
with maximum supervision during the morning hours. The same level of supervision was observed for cases done under GA and RA.
In 8 (3.8%) patients the RA technique failed. In 4 (1.94%) cases anaesthetist was unable to institute RA. In these four cases, two attempts were done by the resident and two by the supervisor before opting for GA. In the remaining 4 (1.94%) patients, it failed after institution either due to incomplete or failed block. All these cases were performed by Year Three trainee residents. The selected regional technique used in these cases was spinal anaesthesia and all were converted to GA.
In addition, there were 6 patients who were given GA to expedite delivery in the presence of working labour epidural. Therefore, overall 14 (6.7%) (6 epidural and 8 spinal) required conversion from regional technique to GA. Eleven of these 14 patients (6 epidural and 5 spinal) had Grade 1-3 CS, while 3 patients had Grade 4 CS. The level of supervision in these cases was complete in 13 (92.8%) patients, while it was independent in 1 (7.1%) case which was performed by resident above level three.
On analysing the work shifts and failed RA, we found that 57% of failed RA happened in morning hours, while 43% in the evening and night shifts.
Discussion
There has been a considerable rise in the rate of CS in UK,4 USA,5 Scandinavian6 and Far Eastern countries.7 This rising trend has also been observed in Pakistan.8 In our institution, where the average rate of delivery is 3500 per year, the rate of CS has increased from 36% to 45% between 2007 and 2010. These rising trends clearly indicate that the technique of anaesthesia for different grades CS forms an important part of safe obstetric practice.
Internationally, obstetric anaesthesia guidelines recommend RA over GA for most CS.9 The primary reason for recommending regional block over GA is the risk of failed intubation and aspiration of gastric contents. The percentage use of GA for caesarean section has become a marker of quality for obstetric anaesthesia service.1 Our prospective analysis showed the use GA to be 63% for Grade a CS, which is more or less comparable with the survey done in UK10 showing a range of 34-68% for Grade 1 CS. We fail to show compliance with the international standard1 for semi-emergency and elective CS, where our rate of GA ranged from 46-51% for Grade 2 and 3, and 44% for elective CS. This is in wide contrast with the UK survey10 which showed the use of GA to range from 11-14% for Grade 2 and 3, and only 2-4% for Grade 4 CS. Our retrospective analysis of 2007, 2008 and 2009 showed trends similar to our current prospective trial, which signifies the hospital\\\'s failure to make any progress in reducing the rate of GA for CS in the last four years.
On analysing the reasons for choosing general anaesthesia, we determined that in 45% of cases, it was done because of patients\\\' insistence. The Cochrane database review of 200611 showed that more women prefer to have GA for subsequent procedures when compared with epidural (odd ratio 0.56, 95% CI 0.32 to0.96, one trial 223 women) or spinal (odd ratio 0.44, 95% CI 0.24 to 0.81, 221 women).
Patient refusal for RA is the most important contraindication for the use of regional technique. Over-persuading a reluctant mother to remain awake is potential cause of post-traumatic stress disorder and litigation leading to several cases in medical negligence practice.12 A National Health Service Litigation Authority between 1995 and 2007 handled 841 anaesthesia-related claims, almost half of which (366/841, 44%) were related to regional anaesthesia.13 Of these, about half (186/366) were related to obstetric anaesthesia and analgesia. A high proportion of claims also referred to inadequate block and pain during caesarean section.13 The United State malpractice suit14,15 and cases of litigation in UK16 related to RA in obstetrics outnumber those related to GA. It has been shown that patients are more aware to disapprove of care provided to them when they have been conscious than when they are asleep.
The Royal College of Anaesthetists second criteria for best practice for failed RA states that fewer than 3% of regional blocks should require conversion to GA.1 Failure of RA is defined in several ways. Objective outcome include conversion to GA,17-19conversion to any different form of anaesthesia,17,20 or pain during surgery.21,22 Intra-operative discomfort during RA for caesarean section is the most commonly cited anaesthetic cause of litigation in obstetric practice.16 Our failure rate of 3.8% (8 /206) is slightly higher than recommended. Our failure rate in emergency CS (Grade 1-3) was 2.4% (5/206) and for elective CS (Grade 4), 1.4% (3/206), is almost reaching the international standard. Literature review has shown variable failure rates. Garry and Davies21 have shown a rate of 8%, while a survey of 14 hospitals in UK reported a conversion of 14.3% of cases.18 Kinsella23 reported a conversion rate of 4.9% in a prospective audit of 5080 caesarean sections, which was reduced to 4.1% if cases were excluded in which GA was given to expedite delivery in the presence of working epidural. If we include patients with labour epidural who were given GA, then our failure rate would be 6.7% (14/206). As all of our conversion of labour epidural was due to time constraint, there is a need to develop a guideline for starting epidural in the labour room.
We also determined the impact of work hours and level of supervision on the choice of anaesthesia. Our prospective analysis did not show any correlation between the choice of anaesthesia and work hours. However, a significant difference was observed in the level of supervision for different work hours, where maximum complete supervision was observed in the morning hours. This showed that the practice of using particular anaesthesia technique remained the same in spite of having less supervision during the evening and night shifts.
The lack of patient awareness and education in our part of the world leads to fear of complication such as paralysis and backache with RA, which has led to a low rate of regional technique in our hospital setting. Besides, patients completely rely on obstetricians to make a decision for their anaesthesia technique. Many obstetricians believe that regional techniques take more time in preparation and administration. In order to change this attitude, a study24 was done to determine that the use of spinal anaesthesia was not associated with decrease intra-operative time efficiency compared to GA for elective CS. We believe that obstetricians can play a major role in changing patient\\\'s attitude towards regional technique. In our survey, we found that in 10% of cases it was surgeon\\\'s choice and it was mostly for grade 2-3 CS. Obstetrician distress has implication for the anaesthetist and may lead to a decision to use general anaesthesia in many cases, when regional anaesthesia could have been the choice. In our audit, 17% of GA cases were because of anaesthetist choice, and mostly it was for grade 2-3 CS. Reasons for anaesthetist choosing GA were failed RA, patients\\\' condition like low platelet, coagulation abnormality and urgency of a case. One survey done in Hyderabad, Pakistan25 showed that 75% of practicing anaesthetists preferred GA for CS.
Although we are far behind the international standard in our technique for regional anaesthesia, by means of studies, regular audits and meetings, we have managed to bring down the rate of GA for CS. In our institution, the rate of GA for CS was 80% in 1997, which has slowly declined to 47% in 2010. We are further trying to educate patients on the advantages of regional technique for CS by brochures and counselling in the pre-operative anaesthesia clinic.
Conclusion
Patient education regarding the use and benefits of RA needs to be enforced. This education needs a positive reinforcement from obstetricians and the nursing staff. Good multidisciplinary communication is crucial to the safe management of women requiring caesarean section. In order to meet the international standards for best practice, guidelines should be made in consultation with the obstetrician and nursing staff regarding the use of RA for different grades of CS. This will help the care-givers to reach a consensus decision for the anaesthesia technique best for the patient.
Acknowledgements
We would like to thank Ms. Yasmeen Surani (Head Nurse, Obstetric Unit) for her support and Mr. Iqbal Azam (Assistant Professor, CHS Department) for his suggestions on data analysis.
References
1. Royal College of Anaesthetist. Technique of anaesthesia for Caesarean section. In: raising the Standard: a Compendium of Audit Recipes. (Online) (Cited 2011 Jan 16). Available from URL: http://www.rcoa.ac.uk/index.asp. page ID=125.
2. Lucas DN, Yentis SM, Kinsella SM, Holdcroft A, May AE, Wee M, et al. Urgency of caesarean section: a new classification. J R Soc Med 2000; 93: 346-50.
3. Caesarean section: clinical guideline. National Collaborating Centre for Women\\\'s and Children\\\'s Health; Commissioned by NICE .London: Royal College of Obstetricians and Gynaecologists Press, 2004.
4. NHS Maternity Statistics, 2008-09. (Online) (Cited 2011 Jan 16). Available from URL: http://www.ic.nhs.uk/statistics-and-data-collection/hospital-care/maternity/ nhs-maternity-statistics-2008-09.
5. Menacker F, Hamilton BE. Recent trends in caesarean delivery in the United States. NCHS Data Brief 2010; 35: 1-8.
6. Dahl V, Spreng U J. Anaesthesia for urgent (grade 1) caesarean section. Curr Opin Anaesthesiol 2009; 22: 352-6.
7. Associated Press. C-section rates around globe at \\\'epidemic\\\' levels. (Online) (Cited 2011 Jan 16). Available from URL: http://www.msnbc.msn.com.
8. Najmi RS, Rehan N. Prevalence and determinants of cesarean section in a teaching hospital of Pakistan. J Obstet Gynecol 2000; 20: 479-83.
9. American Society of Anesthesiologist Task Force on Obstetric Anesthesia practice guidelines for Obstetric anesthesia: an updated report by the American Society of Anesthesiologist Task Force. Anesthesiology 2007; 106: 842-63.
10. Kinsella SM, Walton B, Sashidharan R, Draycott T. Category-1 caesarean section: a survey of anaesthetic and perioperative management in the UK. Anaesthesia 2010; 65: 362-8.
11. Afolabi BB, Lesi FE, Merah NH. Regional versus general anesthesia for caesarean section. Cochrane Database Syst Rev 2006; 4: CD 004350.
12. Reynolds F. Controversies. General Anesthesia is unacceptable for elective cesarean section. Report of a debate held at the Society of Obstetric Anesthesia and Perinatology, 40th Annual meeting, Chicago, USA, May 2008. Int J Obstet 2010; 19: 209-17.
13. Szypula K, Ashpole KJ. Bogod D, Yentis SM, Minai R, Scott S, et al. Litigation related to regional anaesthesia: an analysis of claims against the NHS in England 1995-2007. Anaesthesia 2010; 65: 443-52.
14. Chadwick HS. An analysis of obstetric anesthesia cases from the American Society of Anesthesiologist close claims project data base. Int J Obstet Anesth 1996; 5: 258-63.
15. Ross BK. ASA closed claims in obstetrics: lessons learnt. Anesthesiol Clin N Am 2003; 21:183-97.
16. Ashpole K, Yentis SM, Scott S, Mihai R, Cook TM. NHS litigation authority claims associated with caesarean section. Int J Obstet Anesth 2008; 17:52.
17. Shibli KU, Russell IF. A survey of anaesthetic techniques used for caesarean section in UK in 1997. Int J Obstet Anesth 2000; 9: 160-7.
18. Jenkins JG, Khan MM. Anaesthesia for Caesarean section: a survey in a UK region from 1992-2002. Anaesthesia 2003; 58: 1114-8.
19. Bloom SL, Spong CY, Weiner SJ, Landon MB, Rouse DJ, Varner MW, et al. Complications of anesthesia for cesarean delivery. Obstet Gynecol 2005; 106: 281-7.
20. Riley ET, Papasin J. Epidural catheter function during labor predicts anesthetic efficacy for subsequent cesarean delivery. Int J Obstet Anesth 2002; 11: 81-4.
21. Garry M, Davies S. Failure of regional blockade for caesarean section. Int J Obstet Anesth 2002; 11: 9-12.
22. Habib AS, Dale M, Emerson C, Allsager C, Victoria A, Bourne TM. Reduction in pain during caesarean section following addition of neuraxial Opioids: a close loop audit. Int J Obstet Anesth 2002; 11: S17.
23. Kinsella SM. A prospective audit of regional anaesthesia failure in 5080 caesarean section. Anaesthesia 2008; 63: 822-32.
24. Ismail S, Huda A. An observational study of anaesthesia and surgical time in elective caesarean section: spinal compared with general anaesthesia. . Int J Obstet Anesth 2009; 18: 352-5.
25. Shaikh MS, Sabbar S, Aziz N, Shaikh NB, Akhund T. Acid prophylaxis during anaesthesia for caesarean section. A survey among anaesthetists at Hyderabad. J Ayub M Coll Abbottabad 2009; 21: 87-9.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: