
Haji Khan Khoharo ( Department of Medicine, Muhammad Medical College Hospital, Mirpurkhas, Sindh. )
Abdul Waheed Halepoto ( Department of Medicine, Muhammad Medical College Hospital, Mirpurkhas, Sindh. )
April 2012, Volume 62, Issue 4
Original Article
Abstract
Objective: To evaluate the QTc-interval, heart rate variability and postural hypotension in predicting cardiac autonomic neruopathy (CAN) in type 2 diabetes mellitus (DM) patients
Methods: The comparative cross-sectional study was conducted in the Department of Medicine, Muhammad Medical College Hospital, Mirpurkhas, Sindh, from September 2008 to December 2009. A total of 186 type-2 diabetes mellitus patients with a QTc value of >440 ms were studied. The QT interval was measured on electrocardiographic (ECG) recordings. The patients with HbA1c levels < 7% were considered as well-controlled. A cut-off of 5 years was selected for the known duration of diabetes. The longest and shortest R-R intervals on ECG, and heart rate variability (HRV) were determined. An HRV of less than 20 beats per minute was accepted as CAN. The relationship of postural hypotension (PH) and heart rate variability to the duration and control of diabetes were also evaluated. The relationship of cardiac autonomic neuropathy with diabetes control was also determined. Data was analysed using SPSS 10.0 (Chicago, Illinosis, USA). The comparison of differences in means was calculated by the student t-test and the difference in proportions was compared by the Chi-square test. A p-value of <0.05 was considered significant.
Results: The mean age was 47±13 years, and the mean duration of diabetes was 13±7 years. All cases had QTc prolongation with mean 0.52±0.19. Median QTc intervals were 0.590 (range. 0.515-0.780) and 0.631 (range 0.530-1.869) for males and females respectively. Cardiac autonomic neuropathy manifestations were prominent in diabetics of > 5 years when compared with patients for < 5 years (p < 0.003). The postural hypotension difference increased while the heart rate variation decreased with the duration of diabetes (p < 0.002). The PH on standing was significantly related with the control (p<0.002) as well as the duration of diabetes (p<0.002). Heart rate variation with respiration was significantly related to the duration (p<0.005), but not to the control (p=0.59) of diabetes. QTc showed a significant correlation with the duration of diabetes, postural hypotension and heart rate variation with respiration (p <0.005, p< 0.013, p <0.004) respectively.
Conclusions: Prolonged QTc interval, heart rate variation and postural hypotension are relatively easy, quick and inexpensive methods to measure cardiac autonomic neuropathy.
Keywords: Diabetes mellitus, Heart rate, Postural hypotension (JPMA 62: 328; 2012).
Introduction
Cardiac autonomic neuropathy (CAN) contributes significantly to increased cardiovascular mortality and morbidity in type 2 diabetic patients.1 CAN is a common complication of diabetes and is associated with resting tachycardia, Postural Hypotension (PH), painless myocardial ischaemia or infarction, arrhythmias and sudden cardiac death.2 Lack of Heart Rate Variability (HRV) during deep breathing or exercise is a sign of CAN in patients with diabetes.3 An increased resting heart rate (HR) and loss of Heart Rate Variability (HRV) in response to deep breathing are primary indicators of parasympathetic dysfunction. Tests for sympathetic dysfunction include measurements of HR and blood pressure responses to standing, exercise and handgrip.4 Disturbances of HRV with respiration and PH are the most commonly seen manifestations of CAN among diabetics. The incidence of CAN raises parallel with the known duration of diabetes. Studies have found a positive correlation between the findings of CAN and the known duration of diabetes.5-7 A prolonged corrected QT interval (QTc) indicates an imbalance between right and left sympathetic innervation. Diabetic patients with a regional sympathetic imbalance and QTc interval prolongation may be at a greater risk for arrhythmias. The measurement of QT interval is suggested as a sensitive, non-invasive, and simple predictor of cardiac dysautonomia.8 The aim of the present study was to assess the importance of QTc interval, PH and lack of HRV as a non-invasive method to predict CAN.
Patients and Methods
This comparative cross-sectional study was conducted at the Department of Medicine, Muhammad Medical College Hospital, Mirpurkhas, Sindh, from September 2008 to December 2009. A total of 186 patients were selected through non-probability purposive sampling. Known type 2 diabetics with a QTc value of >440 ms were included in the study. Patients with cardiac drugs intake, cardiac rhythm abnormalities, and heart blocks were scrutinised and excluded from the study. Supine blood pressure after 10 minutes of rest was measured. The BP measurement was repeated after 3 minutes of active standing with handgrip. Differences in systolic blood pressure while in standing and supine positions were noted. A difference of more than 30 mmHg was defined as the presence of PH.5 The variation of heart rates in inspiration and expiration was determined by ECG. The patients were positioned supine (head elevated up to 30 degrees) and asked to inspire for 5 seconds then expire for 5 seconds. This was repeated six times. The longest (minimal HR) and shortest (maximal heart rate) R-R intervals on ECG and HRV (maximal HR - minimal HR) were determined. The variation of HR during inspiration and expiration of less than 20 beats per minute was accepted as CAN.9 The HRV related to respiration does not influence QT interval. Therefore, QT interval was measured on an ECG recorded at rest and corrected for the cardiac cycle length (QTc). The QTc was calculated by the equation of Bazett: QTc [QT interval/RR interval)].10 The patients selected had prolonged QTc; the longer the QTc interval, the more are the chances of CAN. Blood glucose and HbA1c levels were analysed. Patients with HbA1c < 7% were taken as controlled diabetics and >7% as poorly controlled. The duration of diabetes was grouped as long duration (> 5 years) and short duration (< 5 years). The relationship of PH and HRV with respiration, duration and control of diabetes were evaluated. The relations between CAN findings and diabetic control were also determined. The ethics committee of the institute approved the study. Data was analysed using the SPSS version 10.0 for windows (Chicago, Illinosis, USA).The comparison of differences in means was calculated by the student t-test and the difference in proportions was compared by the Chi-square test. A p-value of <0.05 was considered significant.
Results
A total of 186 patients with diagnosed type 2 diabetes were studied, comprising 98 (52.68%) males and 88 (47.31%) females. Of the total, 152 had diabetes for > 5 years, while 34 patients had diabetes < 5 years. Twenty-eight (15.02%) patients had well-controlled diabetes; the HbA1c < 7% whereas 158 (84.94%) had poorly-controlled diabetes; the HbA1c >7%. The mean age noted was 47±13year and the mean duration of diabetes was 13±7 years (Table-1).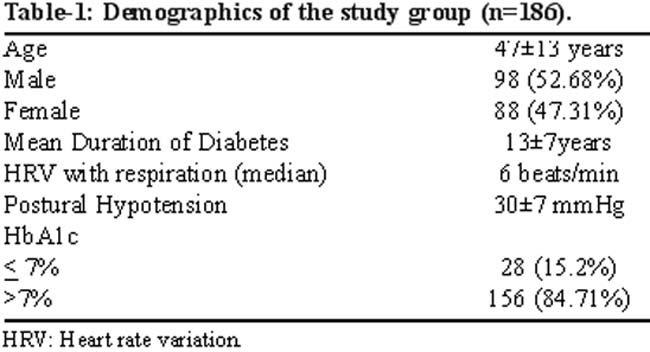
All cases had QTc prolongation with mean 0.52±0.19 (range 0.491- 0.912, median: 0.670). Median QTc intervals were 0.590 (range 0.515-0.780) and 0.631 (range 0.530-1.869) for males and females respectively. There was no statistically significant relationship between categorised QTc values and gender (p=0.650). The comparisons of median PH differences and HRV with regard to diabetic control and the known duration of diabetes were calculated (Table-2).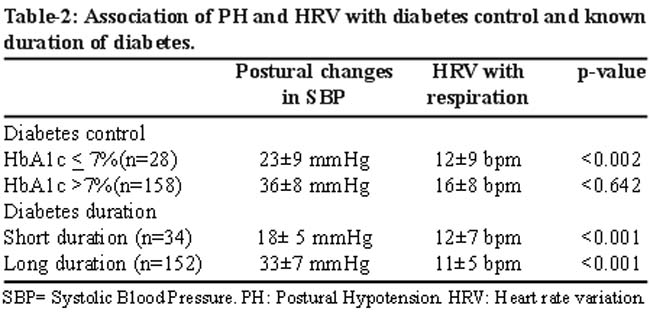
Manifestations related to CAN were more prominent in cases where duration of diabetes was > 5 years, compared to those who were diabetics for < 5 years (p < 0.003). PH differences increased while the HRV decreased with the duration of diabetes (p < 0.002). PH in standing position was significantly related with the control and the duration of diabetes (p<0.002) (p<0.003) respectively. HRV with respiration was significantly related to the duration (p<0.005), but not to the control (p=0.59) of diabetes. QTc showed a significant association with the duration of diabetes, PH, and HRV with respiration (p <0.005, p< 0.013, p <0.004) respectively.
Discussion
The clinical significance of QTc prolongation is determined by its frequency, length and its association with adverse clinical events. CAN was more prominent in cases whose known duration of diabetes was > 5 years, when compared with patients who were diabetics for < 5 years (p < 0.003). The results of previous studies4,8,11 have proved that an abnormal QTc interval is an indicator of sympathetic and parasympathetic nervous system dysfunction and is predictive of increased mortality and decreased survival with ventricular arrhythmias in diabetic patients. Although a controversy exists relating to the upper limit of normal QTc interval, a QT interval >440 ms definitely necessitates an urgent intervention such as a cardiac evaluation or revision of the treatment.12-14 We found patients with CAN-induced QTc prolongation up to 0.912 ms with a median QTc of 0.631ms. The result matches clearly with those mentioned in the literature.11,12,14,15 Although it is relatively easy and quick to measure QTc levels, other signs supporting this serious diagnosis will be useful as well. The findings of a study11 confirmed the prognostic value of QTc interval as an independent risk factor causing mortality in type 2 diabetics. Another study16 has shown that QTc prolongation is an independent risk factor for arrhythmias and cardiac death. The study of Pappachan JM et al17 has shown CAN to be present in 60% of diabetics and QTc prolongation as an independent risk factor for the mortality. The fact that positional changes in systolic blood pressure are significantly affected by the duration and control of diabetes, shows high correlation with the QTc values, and further increases the importance of QTc in the evaluation of CAN. Vagal degeneration causes respiratory changes in HR and leads to tachycardia.16 In our study, HRV related to respiration seemed to be an important predictor of CAN, but this finding should probably be evaluated more cautiously since it is not affected from the control of diabetes alone. Diabetic duration was associated both with HRV (with respiration) and PH, but diabetic control was associated with HRV only. We suggest checking QTc interval, PH and HRV with respiration in patients with a diabetic history of five years or more. However, further studies involving healthy persons and diabetic patients should be performed in order to reveal the effects of indicators in diabetic CAN. Our study had its limitations because it lacked normal healthy persons as a control group.
Conclusions
Prolonged QTc interval, HRV with respiration and PH are relatively easy, quick and inexpensive methods to measure CAN in diabetic subjects. Prolonged QTc interval may cause life-threatening cardiac arrhythmias and even death.
References
1. Odusan O, Familoni OB, Raimi TH. Correlates of cardiac autonomic neuropathy in Nigerian patintes with type 2 diabetes mellitus. Afr J Med Sci 2008; 37: 315-20.
2. Scott LA, Kench PL. Cardiac autonomic neuropathy in the diabetic patient: does 123I-MIBG imaging have a role to play in early diagnosis? J Nucl Med Technol 2004; 32: 66-71.
3. Subbalakshmi NK, Adhikari PM, Rajeev A, Asha K, Jeganathan PS. Independent predictors of cardiac parasympathetic dysfunction in type 2 diabetes mellitus. Singapore Med J 2008; 49: 121-8.
4. Pop-Busui R. Cardiac autonomic neuropathy in diabetes: a clinical perspective. Diabetes Care 2010; 33: 434-41.
5. Khoharo HK, Qureshi F. Frequency of cardiac autonomic neuropathy in patients with type 2 Diabetes mellitus reporting at a teaching Hospital of Sindh. J Coll Physicians Surg Pak 2008; 18: 751-4.
6. May O, Arildsen H, Damsgaard EM, Mickley H. Cardiovascular autonomic neuropathy in insulin-dependent diabetes mellitus: prevalence and estimated risk of coronary heart disease in the general population. J Intern Med 2000; 248: 483-91.
7. Kumhar MR, Agarwal TD, Singh VB, Kochar DK, Chadda VS. Cardiac autonomic neuropathy and its correlation with QTc dispersion in type 2 diabetes. Indian Heart J 2000; 52: 421-6.
8. Lo ss, Sutton MS, Leslie RD. Information on type I diabetes mellitus and QT interval from identical twins. Am J Cardiol 1993; 72: 305-9.
9. Khoharo HK, Ansari S, Shaikh IA, Qureshi F. Cardiac autonomic neuropathy (CAN) in type-1 diabetes mellitus patients and its association with the duration of disease and glycemic control. J Coll Physicians Surg Pak 2009; 19: 232-5.
10. Porwal V, Raman PG. QT interval in diabetes mellitus. Int J Diab Dev Countries 2005; 25: 46-7.
11. Stettler C, Bearth A, Allemann S , Zwahlen M, Zanchin L, Deplazes M, et al. QTc interval and resting heart rate as long term predictors of mortality in type 1 and type 2 diabetes mellitus: a 23 year follow up. Diabetologia 2007; 50:186-94.
12. Aytemir K, Aksoyek S, Ozeer N, Gürlek A, Oto A. QT dispersion and autonomic nervous system function in patients with type I diabetes. Int J Cardiol 1998; 65: 45-50.
13. Vinik AI, Maser RE. Screening for asymptomatic coronary artery disease in patients with type 2 diabetes. JAMA 2009; 302:735-6.
14. Veglio M, Sivieri R, Chinaglia A, Scaglione L, Cavallo-Perin P. QT interval prolongation and mortality in type 1 diabetic patient: a 5-year cohort prospective study. Neuropathy Study Group of the Italian Society of the Study of Diabetes, Piemonte Affiliate. Diabetes Care 2000; 23: 1381-3.
15. Rossing P, Breum L, Major-Pedersen A, Sato A, Winding H, Pietersen A, et al. Prolonged QTc interval predicts mortality in patients with Type I diabetes mellitus. Diabet Med 2001; 18: 199-205.
16. Vinik AI, Maser RE, Mitchel BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care 2003; 26: 1553-79.
17. Pappachan JM, Sebastian J, Bino BC, Jayaparkash K, Kumar V, Suujathan VK, et al. Cardiac autonomic neuropathy in diabetes mellitus; prevalence, risk factors, and utility of QTc interval in the ECG for its diagnosis. Postgrad Med J 2008; 85: 205-10.
18. Kocer AK, Akturk Z, Maden E, Tasci A. Orthostatic hypotension and heart rate variability as indicator of cardiac autonomic neuropathy in diabetes mellitus. Eur J Gen Med 2005; 2:5-9.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: