
Rashid Hashini ( Department of Radiology, Nagasaki University Hospital, 1-7-1, Sakamoto, Nagasaki 852-8501, Japan. )
Masataka Uetani ( Department of Radiology, Nagasaki University Hospital, 1-7-1, Sakamoto, Nagasaki 852-8501, Japan. )
Aamer Aziz ( Department of Radiology, Nagasaki University Hospital, 1-7-1, Sakamoto, Nagasaki 852-8501, Japan. )
Kuniaki Hayashi ( Department of Radiology, Nagasaki University Hospital, 1-7-1, Sakamoto, Nagasaki 852-8501, Japan. )
March 1999, Volume 49, Issue 3
Case Reports
History
A 30 years old female presented with acute onset of right sided chest pain. She had a past history of repeated episodes of pneumothorax the cause of which has not been determined. She was a non-smoker.
Physical examination
On physical examination she was found to be dyspneic. Otherwise examination was unremarkable.
Laboratory findings
Blood counts, ESR, electrolytes, serum total protein, LDH, alkaline phosphatase and renal indices were normal.
Pulmonary function test was as follows:
VC: 2.80L, %VC:89.2%, FEV: 2.25L, FEV1%:79.2%, DLCO/VA:42ml.min.mmHg/L.
With patient breathing room air, arterial blood gas values were as follows: pH:7.397, PaO2:85.lmmHg, PaCo2:43.3mmHg.
Imaging
Chest radiograph (Figure 1)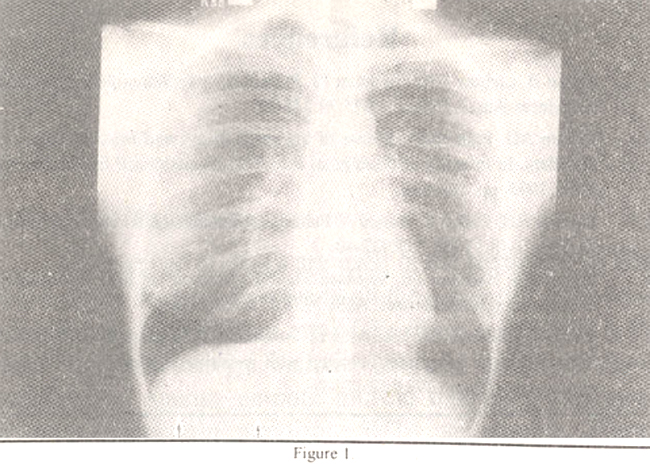
showed lucency in the right lower lung with a air-fluid level (arrows) over the right hemidiaphragm suggesting hydropneumothorax. In addition, diffuse fine reticular opacities were seen in both lungs. Lung volume was increased. Computed tomography (CT) of the chest (Figure 2)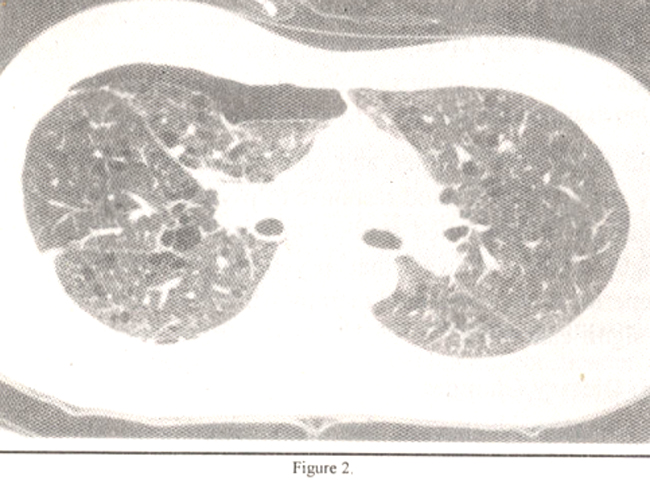
showed multiple thin walled cysts distributed uniformly throughout the lungs.
Diagnosis
Pulmonary lymphangioleiomyomatosis
Disucssion
Lymphangioleiomyomatosis (LAM) is a rare progressive disorder, of unknown cause, that primarily affects women during their childbearing years. It is characterized by diffuse hyperplasia of atypical smooth muscles in the walls of bronchi, bronchioles, alveolar septa, pulmonary vessels, lymphatics and pleura1.
The initial manifestations include progressive dyspnea, pneumoth orax, chy lothorax or hemoptysis. Pneumothorax as an initial event is common and often recurs. Pulmonary function tests usually show airflow obstruction, increased total lung capacity, increased compliance and impaired diffusion.
Earliest radiographic signs consist of fine nodular, reticular or reticulonodular opacities. With time the reticular pattern tends to become coarser and more irregular. Cysts, bullae, and honeycombing may develop. At this stage lung volumes commonly increase. The combination of interstitial opacities and increasing lung volumes is characteristic of LAM, as opposed to the progressive loss of volumes that accompany most other interstitial diseases2. These radiographic findings may precede, accompany, or postdate other radiological findings such as pneumothorax and chylous pleural effusion.
Chest CT findings in LAM are very suggestive, if not specific, for this disease3. In over 80% of the patients, CT shows multiple, thin walled cysts of various diameters which are distribtued diffusely in otherwise normal lung. No portion of the lung is spared. Cysts are clearly demarcated by a thin wall and are of variable size. Although the cysts are identifiable on conventional CT, high resolution CT (HRCT) adds confidence to the diagnosis. Mediastinal lymphadenopathy is usually associated with LAM.
CT features similar to that seen in LAM can also be seen in pulmonary eosinophilic granuloma (H istiocytosis X). However, in most patients with EG a nodular component is also present. Furthermore, EG characteristically involves upper two-thirds of the lungs and spares the costophrenic angles, while lymphangioleiomyomatosis involves the lungs diffusely4. Cystic air spaces are common in a variety of fibrotic interstitial lung disease particularly end stage idiopathic pulmonary fibrosis (IPF). However, the distribution of abnormalities and absence of findings of severe fibrosis in patients with LAM allow their differentiation.
The pulmonary changes in LAM are histologically and radiogrphiclly identical to those of pulmonary tuberous sclerosis. However, the relationship between these two diseases is not clear. LAM develops in approximately 1% of the patients with tuberous sclerosis. It differs from pulmonary tuberous sclerosis in that it is not heredofamilial and lacks many of the neuroectodermal features of pulmonary tuberous sclerosis such as adenoma sabeceum, epilepsy and mental retardation.
LAM is ususally progressive and patients die of respiratory insufficiency. Treatment has consisted of radiation therapy, surgical ablation of the thoracic duct, removal of involved lymph nodes and pleurodosis to decrease the pneurnothoraces and chylous pleural effusion; however, these all have been largely unsuccessful. After the identification of estrogen and progestin receptors in the lungs of patients with LAM, various types of hormonal therapy (antiestrogens, medrooxyprogesterone, bilateral oophorectomy etc.) involved lymph nodes and pleurodosis to decrease the pneumothoraces and chylous pleural effusion; however, these all have beeen largely unsuccessful. After the identification of estrogen and progestin receptors in the lungs of patients with LAM, various types of hormonal therapy (antiestrogens, medrooxyprogesterone, bilateral oophorectomy etc.) have been employed with varied degree of success5. In few cases heart-lung transplantation has also been conducted. However, no treatment is currently considered as ideal and overall prognosis is generally poor.
Acknowledgement
Thanks to Mr. Y. Hayashida for his assistance in development and printing of photographs.
References
1. Corrin B, Liebow AA, Friedman PJ. Pulmonary lymphangioleiomyomatosis: A revieew. Am. J. Pathol., 1975;79:348-82,
2. Wilson AG. Pulmonary disease of unknown origin and miscellaneous lung disorders. In Imaging of diseases of the chest. Armstrong P Ed. Mosby year book. 1995, pp. 568-608.
3. Sherrier RH, Chiles C, Roggil V. Pulmonary lymphangioleiomyomatosis: CT findings. AJR., 1989;153:937-40.
4. Bonelli FS, Hartman TE, Swensen Si, et al. Accuracy of high resolution CT in diagnosing lung diseases, MR. 1998;170:1570-72.
5. Urban 1, Kutten F, Gompel A, et al. Pulmonary lymphangioleiomyomatosis. Follow-up and long term outcome with antiestrogen therapy - a report of eight cases. Chest, 1992;l02:472-76.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: