
Riaz Qureshi ( Family Medicine Division, The Aga Khan University, Karachi. )
January 1999, Volume 49, Issue 1
Family Medicine Corner
Care of the dying (terminal care; palliative care) is considered to be the active total care ofpatients whose disease is not responsive to curative treatment1,5. The goal of this care is achievement of the best possible quality of life for patients and their families. Most patients would like to die in familiar surroundings, at home2.
Control of all symptoms including pain, psychological, social and spiritual problems are imperative. A kind, caring attitude of a Family Physician is as important as the medication be prescribed.
Principles of a Family Physician’s Role in Terminal Care3 A structured strategy with the following principles is most likely to achieve the best possible quality of life for the terminal care patients.
1. Symptom control and relief
2. Communication with the patient - never isolate the patient
3. Avoidance of inappropnate therapy
4. Support of the relatives
5. Teamwork - with nurses, social workers, physiotherapists and relevant specialists
6. Continuity of care - regular visiting by the doctor and nurse
Symptom Control
- Ensure that the patient and family are aware that pain will be controlled; there is a great fear of pain and a painful death.
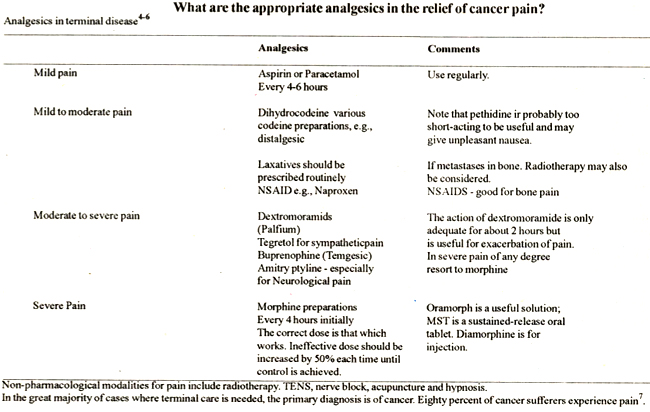
- Start analgesia early, regularly and in appropriate dose. Anticipate the next wave of pain by regular dosage.
Analgesics are always more effective in preventing the development of pain than in the relief of established pain.
- Do not be afraid of opiates, drug dependency or large doses; give sufficient for the patient’s needs.
- Remember there are other techniques, e.g., nerve blocks. Do not be afraid to consult experts.
- Control other symptoms, e.g., constipation, cough, dyspnoea, insomnia.
Communication
- Above all give the patient time to talk of his fears and his problems.
- Be honest and truthful if questioned, but not pessimistically so.
- A policy of ‘gentle truth’ is generally best.
- Adopt a kind, sympathetic approach; do not be afraid to touch the patient.
- Respect his religious convictions.
- Never say, ‘There is nothing more! can do’.
- Don’t raise false hopes, but reassure that symptoms will be relieved.
Avoidance of Inappropriate Therapy
Consider the time and question the need for any invasive palliative measures such as intravenous infusion, etc. Respect the patient’s wishes.
Support of the Relatives
- Help the fanuly in caring for and in communicating with the patient; above all involve them in the patient’s care.
- Explain the prognosis and symptomatic treatment clearly.
- Answer their fears and try to alleviate problems. Do not overlook possibilities of financial help.
- Give support with nursing problems, etc.
- Try to avoid a ‘conspiracy of silence’ between family, patient and doctor.
- Try to reduce any feelings of guilt within the family by showing understanding.
Team Work
Involve one or more members of the team, night nurse, lady health visitor, home help, occupational therapist, social worker, etc; do not forget an appropriate religious and relevant hospital specialist help.
Continuity of Care
- Ensure that the patient and relatives know that someone will always be available night and day to help, if needed.
- Visit regularly to provide support.
- Do not charge any fee from non-affording patients.
What are the problems of telling the patient the diagnosis and prognosis of his illness?3
This is a difficult question to answer. Each patient will require an individual assessment and management. It is important to find out how much the patient knows about his/her illness by asking about his/her knowledge of the disease, his/her ideas, concerns and expectations.
Keeping the patient un-infonned about his illness often causes excessive emotional strain on the family and the carers, including the physician. A knowledge of his/her prognosis may help the patient to plan forwhatevertiine he/she may have left and also for the future of his/her family.
A difficult situation arises when the relatives wish that the patient should not find out the true nature of his/her illness. A gentle persuasion of the family to tell the patient the truth may be worthwhile.
Another difficult problem arises when the patient does not want his family to know about his illness. Again a gentle persuasion that it may be in his/he and his/her immediate family’s best interest that the knowledge of the true nature and prognosis of the disease is equally shared, is the best option.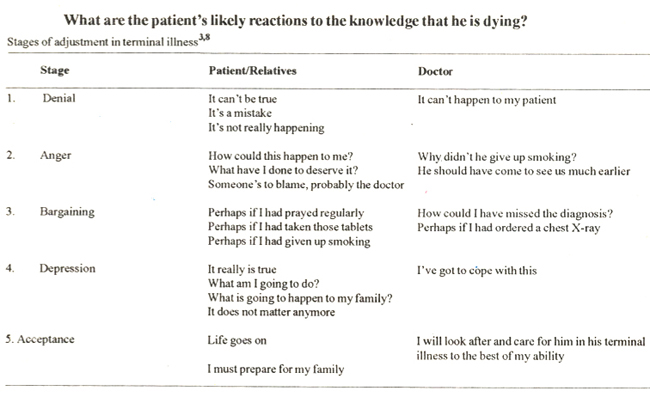
In exeptional circumstances when a patient indicates that he/she does not want to know the nature and prognosis of his illness, his/her wishes should be respected.
Other common symptoms, which may need attention, include nausea/vomiting, constipation, diarrhoea, cough, dyspnoea, mouth problems, depression, confusion/anorexia, fungating tumors. Appropriate therapies for these symptoms form an integral part of good quality terminal care.
The Advantages and Dis antages of Trying to Manage a Dying Patient at Home2,3,8
It is not useful to make dogmatic assertions that all patients should die at home or indeed in hospices; much depends on the individualand the circumstances at the time.
InUK about one-third of patients die at home, two-third in hospital and 5% in non-National Health Service (NHS) hospitals or hospices. According to a UK study if home circumstances had allowed, two third of terminal care patients expressed a preference to die at home.1,8
Home
The factors that usually determine whether home care is feasible are:
(a) The Patient Does he wish to? (Some feel they will be too great a burden to their families).
Are there any important medical needs lie can only receive in hospital?
(b) The relatives How many are there?
Do they feel they can cope?
Can they look afterthe patient at night?
The financial implications of Hospital Care.
(c) The services available Are night nurses available? Any other Nurses.
Are bedpans, comniodes, etc. available?
Hospital
Care may often fall below desirable levels here for a variety of reasons. Sometimes death is regarded as a failure.
The staff may be busy. Analgesia should be no problem, but an alarmingly high proportion of patients still die in pain even in hospital.
Conspiracy of Silence8
The relationships between the carers and the patient are some time clouded with lies and deceptions. A Fanuly Physician’s important role is to get the patient and the carers to talk about their fears and feelings.
Hospice/Terminal Care Units
The staff in these units are specialists in symptom control and a positive commitment to the patients with an individual approach ensures some of the veiy best of terminal care. Very few such units are available in Pakistan.
Following the death of the Patient what more can the Doctor do?
Home care of the tenninally ill is a very valuable preparation for bereavement and at least one study shows that mortality among the bereaved is less if the death occurred at home. Follow-up care of the relatives is essential.
Conclusions
1. Tenninal care at home is one of the most important areas of Family Practice.
2. Analgesia must be regular and appropriate. Morphine is best for severe pain. If Morphine is not available, they Buprenorphine (Temgesic) sublingual may be tried as an alternative.
3. A kind, caring approach by the doctor is as beneficial as the medication he prescribes.
4. Ateamapproach- family practice team working with specialists at relevant stages may provide the best possible care at home.
5. The care of grieving relatives is very important; terminal care does not end with the death of the patient.
References
1. Finlay I, Forbes K. Symptom control in palliative care.Updatc 1 994;48: 180-88.
2. Townsend J, Frank AO. Fermont D. Terminal care and patients preference fbr place of death.
3. Mead M, Patterson H. Terminal care in general practice; Tutorials in general practice 1992.
4. Prescribing in Terminal Care. British National Formulary No. 22, September, 1991.
5. Cancer pain relief and palliative care, Report of a WHO Expert Committee. Geneva, WHO, 1990 (Technical Report Series No.804).
6. Palliative Cancer Care Guidelines, Scottish Partnership Agency with the Clinical Resources and Audit Group, January. 1994.
7. Mersey Drug Information Service and the Department of Pharmacology, University of Liverpool. Care ofthe dying drug information, Letter. Me.Re.CP., 1991.
8. Warren E. Terminal care at home. Postgraduate Tutorials in General Practice 1995, pp. 90-102.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: