
Zeba Aziz ( Department of Medical Oncology, Allama Iqbal Medical College, Lahore. )
Amjad Rehman ( Department of Medical Oncology, Allama Iqbal Medical College, Lahore. )
M. Akram ( Department of Medical Oncology, Allama Iqbal Medical College, Lahore. )
Asif Saeed ( Department of Medical Oncology, Allama Iqbal Medical College, Lahore. )
January 1999, Volume 49, Issue 1
Original Article
Abstract
Objective: Non-Hodgkin\\\'s Lymphosnas (NHL) are common in Southeast Asia, Middle East and Africa. The study was primarily undertaken to establish the demographic and clinicopathologic features of NHL in Pakistan. A secondary aim was to determine the applicability of the International Prognostic Index (IPI) developed by the international lymphoma task force in a developing country.
Methods: A retrospecitve and prospective analysis was performed on 175 patients over 14 years age who presented to the Department of Oncology between August 1994 and December 1996. All patients underwent initial staging according to Ann Arbor Staging System. Histopathologic classification was done according to the International Working Formulation. The IPI was applied to patientswith aggressive lymphornas and age adjusted index to patients <60 years, complete remisioss (CR), disease free survival (DFS) and overall survival (OS) were calculated.
Results: All 175 patients were evaluable. Median age of our patients was 45 years. Male to female ratio was 1.9:1. Seventeen (9.7%) patients were classified as low grade lynthoinas while 158 (91.3%) had intermediate and high grade NHL. Large cell lymphoma was present in 30.9% patients. CHOP (cyclophosphamide 650 mg/m2 day 1, vincristine 1.4 ing/m2 day 1, doxorubicin - 45 mg/m2 day 1 and prednisone 100 mg/rn 2 day 1-5) was the most comon chemotherapy regimen used. Advanced stage (74.9%)> B symptoms (51%) and extranodal involvement (74.3%) were present. One hundred sixty-seven patients were evaluable for response of which 42.8% achieved CR. Median DFS was 19 months and median OS was 22 months.The IPI was applicable to 153 patients and age adjusted IPI to 124 of 153 patients.
Conclusion: Aggressive histology, extranodal diseases, B symptoms and advanced disease are common. International index and age adjusted international index predicted outcome accurately in various risk groups (JPMA 49:11, 1999).
Introduction
Non-hodgkins lymphornas is a diverse group of neoplastic diseases, the incidence of which is rising worldwide by approximately 4% every year. InUS it accounts for only 5% of all newly diagnosed cancers1,2. Available epidemiological data from various parts of Asia indicate marked geographical variation in the incidence, histopathological and clinical behavior of NHL3-6. The disease appears to be more cominonindevelopingcountnes7,8 where a combination of environmental, infectious and genetic factors affect the development of these disorders. Data on various aspects of NHL from developing countries including risk stratification according to IPI, response to treatment and survival are scant)’. Advanced disease, B symptoms and aggressive lymphomas am reportedly more frequent in developing countries. In Pakistan, there are no population based tumor registries, available infonnation is based on hospital based cancer registries . NHL is the most coinon male tumor in Northern Pakistan9.
A retrospective and prospective analysis was conducted between August 1994 and December 1996 on 175 patients with NHL on clinical features, histopathological classification, patient stratification according to the IPI. response to therapy and data.
Patients and Methods
One hundred and seventy five patients with NHL over 14 years of age presenting to the Department of Oncology between August 1994 to December 1996 were evaluated. All patients underwent an initial staging workup according to the Ann Arbor System. This included a complete hematological, renal and hepatic profile. Semm lactic dehydrogenase (LDH), uric acid were also determined. Radiological investigations included chest X-rays, abdominal and pelvic ultrasounds. CT/MRI scans were done when necessary. In case of gastrointestinal symptoms upper GI series with small bowelf ollow through or barium enema were carried out. Bilateral bone marrow aspirates and biopsies were done routinely on all patients. Histopathologic diagnosis was made on the basis of International Working Fonnulation and divided into low, intennediate and high grade. The patients were also classified acconding to the International Prognostic Index for NHL Chemotherapeutic regimens administered included CHOP (Cyclophosphamide Adriamycin Prednisolone Vincristine), BACOP (Bleomycin Adriamycin Cyclophosphamide Predmsolone Vmcristine), CVP (Cyclophosphainide Vincristine Prednisolone), ProMACE (Procatbazine Methotrexate Adriamycin Cyclophosphamide Etoposide) and Cytoboin (Table I).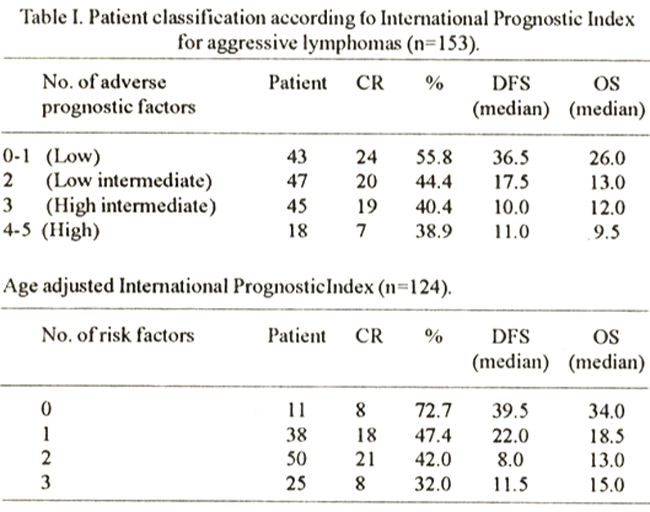
Radiotherapy was given for palliation or bulky disease. All patients underwent repeat staging after therapy ended. Complete remission has traditionally been defined as the disappearance of all clinical evidence of active tumor for a minimum of four weeks. A partial remission was indicated by a decrease of more than 50 percent in the sum of the products of the maximal perpendicular diameters of the measured lesions, lasting at least four weeks. Disease progression was indicated by the appearance of new lesions or by a 25 percent increase in the size of pre-existing lesions.
Results
One hundred and seventy five patients above the age of 14 years presenting to the department between the above mentioned dates were evaluable. Male female ratio was 1.9:1. Median age was 45 years (range 14-80 years). The patient profile is presented in Table II.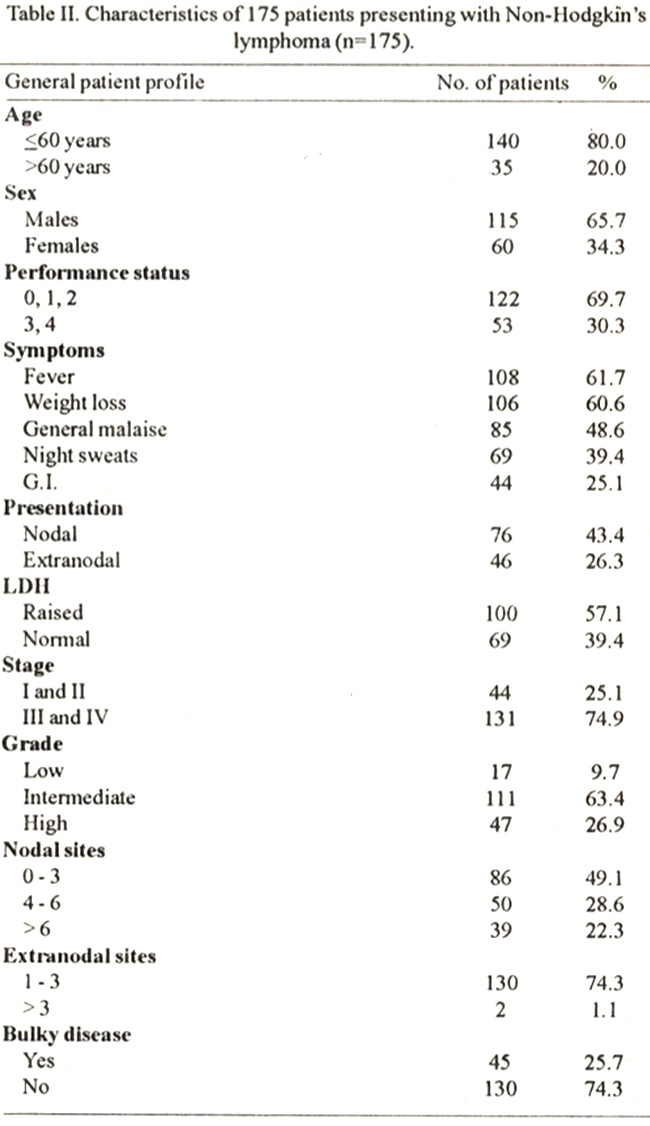
Stage III and IV disease was present in 75% patients. Approximately 65.7% patients belonged to poor socioeconomic status (median per capita income less than US$240).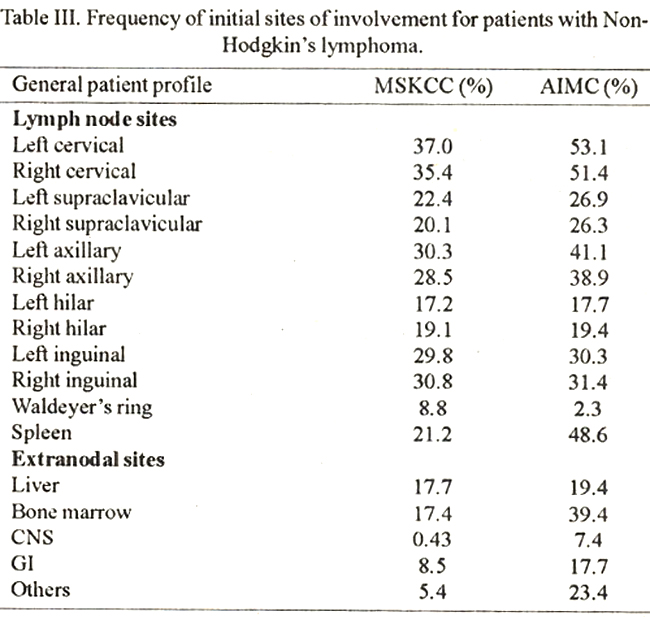
Table III indicates initial sites of involvement. Cervical lymphadenopathy was most common followed by axillaiy involvement. Most common extranodal organ involvement were of bone marrow 69(39.4%), liver 34 (19.4%), gastrointestinal tract which includes stomach, small and large intestines in 13 (17.7%) and central nervous system in 13(7.4%). Bone, kidneys, lung, cervix, skin andbreastwere the areas of extranodal involvement in 45(23%) cases.
Histopathological classification
All histopathology was reviewed by two independent pathologists.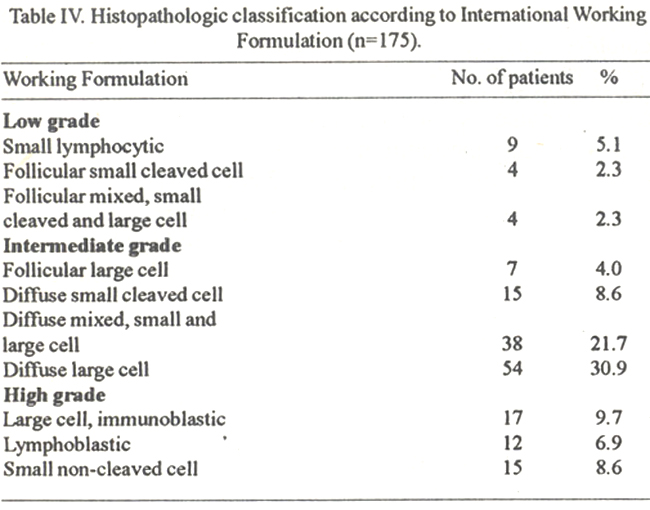
Table IV lists the details of histopathologic classification according to the Working formulation. Majority of the patients (63.4%) belonged to intennediate Non Hodgkin’s lymphonia. The most common subtype of NHL was diffuse large cell accounting for 30.9%.
International Prognostic Index
This was applied to 153 patients with intermediate and high grade NHL on whom data was available on age, LDH, perfonnance status, stage and extranodal involvement as seen in Table IV. Patients were categorized as being at low, low-to-intermediate, intermediate-to-high, or high risk on the basis of the number of unfavorable risk factors present:
Patients with no risk factor or one risk factor were considered to be at low risk, those with two factors were at low-to-intermediate risk, those with three factors were at intermediate-to-high risk and those with four or five factors were at high risk. Them were 140 patients <60 years but the age adjusted model could be applied to only 124 patients on whom complete data was available. Complete remission, overall survival and disease free survival was calculated according to the number of adverse prognostic factors.
Chemotherapy Regimens
The most common chemotherapy regimen used was CHOP in 89 (50.8%) patients with intermediate and high grade lymphoma. CHOP was given foreight courses followed by radiation therapy to bulky disease when necessaiy. Other regimens included m BACOD, ProinaceCYTABOM etc. For low grade NHL chloainbucil/predmsone and CVP were used. Dose modifications and delays were made according to standard international practices for hematological and non hematological toxicities.
Response to treatment
Survival infonnation was available on 167 patients of which 75 (42.8%) patients achieved complete remission. Seventy (40%) patients achieved PR while SD was seen in 3 patients. Progressive disease was present in 19 (10.8%) patients and 8 patients were inevaluable for response.
Median disease free survival was 19 months (range 4-124 months). Overall survival ranged from 1 month to 193 months with a median survival of 22 months. Ninety-six patients have died. Of these 71 patients died due to progressive disease, 16 patients had treatment related complications especially febnle neutropenias. Death due to unrelated causes occurred in six patients and the cause of death is unknown in6 patients. Twenty-six patients are lost to follow-up (Table V).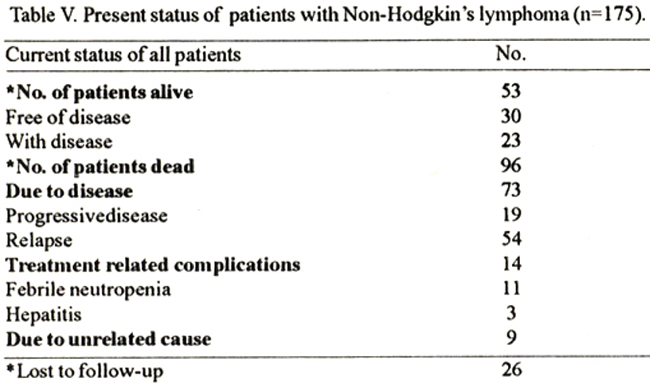
In patients with aggressive lymphomas CHOP was given to 88 patients of which 51% went into CR. Median DFS with CHOP forstage I and II was 17 months (4-71 months) and for stage Ill and IV 12 months (2-66 months).
IPI was applied to all patients belonging to intennediate and high grade lymnphomas and also for patients less than 60 years as seen in Table III. Remission rates, DFS and OS were also calculated according to the international prognostic index. Data on patients with indolent lymphomas was not calculated due to their small number.
Toxicities
In patients with aggressive NHL grade III and IV granulocytopenia developed in 46 subjects receiving CHOP. Grade IV hematological toxicity and febrile neutropenia occurred in 27 patients of which 11 expired; In ten of these cases treatment for febrile neutropenia was delayed by more than 48 hours due to late reporting to the hospital. One patient presented with severe sepsis and shock. Non hernatologic grade Ill toxicities were mnucositis in 2 1.7% and diarrhea in 7.4%. Four patients had exacerbation of their preexisting hepatitis B infection and two of these died in hepatic failure due to fulminent hepatitis.
Discussion
Non Hodgkin’s lymphoma is a major health problem throughout the world. Despite its remarkable sensitivity to chernotherapeutic and radiotherapeutic interventions NHL remains a lethal disease. To our knowledge there is no comprehensive study from the developing countries correlating the IPI with OS and DFS.
Analysis of our data revealed important geographic differences in histopathologic patterns, clinical presentations and survival. The largest published data from Pakistanis from The Armed Forces Institute of Pathology and NHL was the most common tumor in males9,10. This is similar to reports from other parts of Asia and making NHL one of the most frequently occurring cancers in these countries. NHL tends to beadisease of older age inEurope and North Ameriqa. The median age of onset is 65 years withapproximately 60.8% patients beingdiagnosed at>60 years2. This data is at variance from that reported from South East Asia. Earlier reports from Northern India7 and Southern Punjab13 reveal the median age for NHL to be between 40 to 45 years. This is similar to our experience where the median age of our patients is 45 years with only 24.5% patients presenting at 60 years or older. The disease is more common in males however there is significant difference in the male female ratio invarous series. Data from developed countries14 report a male female ratio of 1.4:1 while from developing countries the ratio ranges from 4.5:1 to 3:113,15 In ourseries the ratio is 1.9:1 tending to be inbetween the two groups. The variability in the sex ratio may be partly accounted for by the fact that our society is a male dominated, especially in rural areas and women may not be brought for treatment at all. This scenario is gradually changing and is less common in uiban areas. Advanced disease, B symptoms, bulky disease and number of extranodal sites involved were also much higher in our series than reported from US16. Gastrointetinal involvement was similar to that reported from Japan17 and from North Punjab9.
NHL was classified using the Working Fonnulation based on morphologic features and divided in low, intermediate and high grades. Histology generally followed a reasonable distribution as reported in literature except for low grade lymphomas. Low grade or follicular NEIL is more common in USA18,19 accounting for 25-30% of newly diagnosed cases. Follicular lymphomas are uncommon in developing countries as reported by various series from other parts of Asia, the incidence ranging from 3.4% to 13%5,20,22. In our series low grade NHL was 9.7%. Various possibilities have to be considered including advanced stage of disease which is associated with decreasing nodularity23. The diagnosis may be delayed due to initial treatment for tuberculosis by the general practitioner. This may result in transfonnation from follicularto diffuse variety in some cases, about 14.2% patients presented to us more than 8 months after development of symptoms. Low life expectancy may be another reason as the median life expectancy in Pakistan is 61 years and low grade lymphoma being a disease of the elderly. In addition there may be several unrecognized factors including enviromnental factors e.g., viruses, indiscrIminate use of pesticides and genetic factors making the population more susceptible to diffuse histology.
CHOP is the most common chemotherapeutic regimen used in aggressive NHL. The reasons for this are manifold. Several published randomized trials have shown that overall survival and disease free survival with CHOP were not
significantly different from other aggressive third generation combination therapies24,25. The rate of severe toxic reactions and cost of the drugs is substantially lower. Pakistan is a developing country with limited resources. The average per capita income is 240 US dollars. There are no health insurances and the entire cost of treatment is borne by the patients. In addition, there are few cancer centres, making frequent visits to the hospital difficult for the patients. CHOP therefore despite limitations, is an ideal choice in our countmy. CHOP was administered to 88 patients of which 50.2% patients achieved CR, however, overall survival and disease free survival are somewhat inferior than reported24. The treatment cycles were delayed in majority of our patients for various reasons which included more grade Ill and IV hematological and non-hematological toxicities probably related to poor nutritional status in our patients. Another reason could be that the catclrnient area we serve is approximately 300 square miles as a result of which it is difficult for patients to come on time for the next cycle. These problems are compounded by illiteracy and poverty. The resultant decrease in dose density in our patients may be reflected in relatively poor overall and disease free survival. The international prognostic index was applied to all patients with aggressive lymnphomas and age adjusted index was applied for patients <60 years. CR, DFS and OS were somewhat lower than reported in various series from US26, however, the predictive model was still applicable to our patients.
Eleven of the 27 patients presenting with grade IV febrile neutropenia expired. This high tratment related mortality occurred due to delayed presentation after more than 48 hours of onset of fever. Majority of these patients lived more than 100 kin away and they were treated inadequately by their local physicians. There is now increasing awareness of this problem among the patients and the mortality due to febrile neutropenia has decreased in the last 12 months. Fulminanthepatic failure occurred in three paitents who were hepatitis B positive.
We would also like to comment on enviromnental problems inourcountry which may result ma relatively higher incidence of NHL27. The disease appears to be more common inpatients belonging to poor socioeconomic status. It has been shown that after certain viral infections the virus persists in the host indefinitely either through latency orcontinuous low viral replication. Bacterial, viral and plasmodial infections are common in our country due to lack of clean water supply and poor sewage disposal. EBV28,29 and malaria27 is rampant especially in the lower socioeconomic group. Excessive use and exposure to phenoxyacetic herbicides, organic solvents particularly chlorinated hydrocarbons, TCDD and DDT have all been reported to cause T cell impairment30. We have an agrobased economy and the use of pesticides is very common without scientific know how by the fanners. Lastly malnutrition of expectant mother, fetus and growing children ranged between 40 to 60%. The resultant impainnent of T cell function causes unregulated and sustained B cell response.31
There may be a consequent genetic accident resulting in translocation of c-myc pmtoncogene from chromosome to chromosome18 and.formation of immortalised B cell clone. This comes close to the two hit or multi hit theories of lymphogeneses. Thus critical interaction between host and environmental factors the latter of which may be infections leading to immunologic distuEbances together with rampant malnutrition may account for differences in presentation and increased occurrence of NHL in developing countries.
References
1. Weisenburger DD. .Epidemiology of non-Hodgkin’s lymphoma. Recent findings regarding an emerging epidemic. Ann. Oncol., 1994:15:19 (Suppl I).
2. The National Cancer Data Base Report on Non-Hodgkin’s Lymphoma: Cancer, 1997,80:2311.20.
3. Parkin DM (ed). Cancer occurrence in developing coutnries. IARC Scientific Publication No.75, Lyon International agency for research in cancer. Cancer, 1986;196-231.
4. Intragumtornchai T, Wannakrairoj P, Chaimongkol B, et at. Non-Hodgkin’s lymphomas in Thailand. Aretrospectivepathologic andclinical analysis of l 391 cases. Cancer, 1996;78:1813-19.
5. MX, Li W. Malignant lymphoma in Beijing. J. Environ. Pathol. Toxicol. Oncol., 1992;1 1:327-9.
6. Chi JG, Shin SS, Ahn OH, et at. Malignant lymphomas in Korea. Jpn. J. Clin. Oncol.., 1985;15:653.
7. Obafunwa JO, Akinsete I. Malignant tymphomas in Jos. Nigeria. A ten year study. Cent. Aft. J.Med., 1992;38:17-25.
8. Jussawalla DJ, Gangadharan P. Epidemiology of cancer in the Indian subcontinent, series IV. Indian J. Cancer, 1974; 11:3-11.
9. Azar HA. Cancer in Lebanon and the Near East. Cancer, 1962; 15:66-78.
10. Ahmad M, Khan AH, Mansoor A. The pattern of malignant tumors in Northern Pakistan. AFIP monograph No. I, Rawalpindi, Armed Forces Institute of Pathology, 1990.
11. Pakistan Medical Research Council. Report of multicentre study on malignant tumors. Islamabad, 1982,pp. 5-.-7.
12. Piankijagum A, Pacharee P, Wasi P. Malignant lymphomas in Thailand. An analysis of 1095 cases. J. Med. Assoc., Thai., 1980;63:181-91.
13. Abrar A, Sadaqat AG. Non-Hodgkin’s lymphoma in South Punjab. Retrospective analysis of 148 patients. Pak. J. Med. Res., 1989,28:223-31.
14. About Nasr AL, Tawfik HN, Abu El Einen M. Lymphoreticular tumors and leukemias in Egypt. J. Natl. Cancer, Inst., 1973;50:1619-2 1.
15. Garg A, Dawar R, Agarwal V, et al. Non-Hodgkin’s lymphoma in Northern India. A retrospective analysis of 238 cases. Cancer, 1985;56:972-71.
16. David J, Straua MD, Daniel A, et al. The Non-Hodgkin’s lymphomas. A retrospective clinical and pathologic analysis of 499 cases diagnosed between 1958 and’1969. Cancer, 1983,51:101-9.
17. Philip S. Etias A, Charrles A, et al. Non-Hodgkin’s lymphomas in the Middle East, A study of 417 patients with emphasis on special features. Cancer, 1986;58:1 162-66.
18. Kadin ME, Berard CW, Nanba K, et at. Lymphoproliferative diseases in Japan and Western countries. Hum. Pathol., 1983;14:745.
19. Gallagher CJ, Gregory WM, Jones AE, et at. Follicular lymphoma: Prognostic factors for response and survival. J. Clin. Oncol., 1986;4: 1470-80.
20. Rosenberg SA, Berard CW, Brown BW, et at. National cancer institute sponsored study of classification of non-Hodgkin’s lymphoma: summary and description of a working formulation for clinical usage. Cancer, 1982;49:2112-35.
21. Bosco J, Cherian R, Lin HP, et at. Leukemia and lymphoma in Malaysia. Leuk. Res. 1985;9:789.
22. Ho FCS, Todd D, Loke SI, et at. Clinico-pathological features of malignant lymphornas in 294 Hong Kong Chinese patients: Retrospective study covering an eigh-year period. Int. J. Cancer, 1984;34: 143.
23. Magrath IT Malignant Non-hodgkin’s lymphoma. In Pizzo PA, Poplack DG. (eds). Principles and practice ofpediatric oncology. Philadelphia, JB Lippincott, 1989, p.415.
24. Richard!, FisherMD, Ellen R, et al. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced Non-Hodgkin’s lymphoma, N. Engl. J. Med., 1993;328:1002-6.
25. Gordon LI, Harrington D, Anderson J, et at. Comparison of a second generation combination chemotherapeutic regimen (m-BACOD) with a standard regimen (CHOP) for advanced diffuse Non-Hodgkin’s lymphoma. N. EngI. J. Med., 1992;327: 1342-49.
26. International Non Hodgkin’s Lymphomas Prognostic Factor Project. A predictive model for aggressive Non-Hodgkin’s lymphoma. N. EngI. J. Med., 1993;329:987-94.
27. Parkin DM, Sohier R, O’Connor GT. Geographical distribution of Burkitt’s lymphoma. In: Lenior GM, O’OConor GT and Olweny CLM (eds). Burkitt’s lymphoma. A human cancer model. Lyon: International agency for research on cancer. IARC, IARC Science Publication No.60, 1985, pp. 155-64.
28. Datldorf G. Lymphomas in African children with different forms of environmental influences. JAMA., 1962; 181:1026.
29. Klien G. The Epstien Barr Virus and neoplasia. N. EngI. J. Med., 1975;293 :1353-57-.
30. Vineis PD, Amore F. The role of occupational exposure and immunodeficiency in B cell malignancies. Working Group on Epidemiology of hematolymphopoetic malignancies in Italy. Epidemiology, 1992;3:266-70,
31. Chandra RK. Rossettes forming T cells and cell mediated immunity in malnutrition. Br. Med. J,, 1974;2:608-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: