
TanveerAnjum Chaudhry ( Section of Ophthalmology, Department of Surgery, Aga Khan University, Karachi. )
Tahreem Aman ( Section of Ophthalmology, Department of Surgery, Aga Khan University, Karachi. )
Farheen Shaikh ( Section of Ophthalmology, Department of Surgery, Aga Khan University, Karachi. )
Khabir Ahmad ( Section of Ophthalmology, Department of Surgery, Aga Khan University, Karachi. )
January 2012, Volume 62, Issue 1
Case Reports
Abstract
The case of a 40-year-old-man who presented to our clinic with bilateral blindness as a consequence of bomb blast injuries is reported. He had a completely opaque cornea, partially damaged posterior segment and perception of light in the right eye, while a clear cornea, totally damaged posterior segment and no light perception in the fellow eye. His corneas were successfully swapped which gave him navigational vision.
Keywords: Penetrating keratoplasty, Cornea, Autograft, Contralateral,trauma,
Introduction
Corneal scars in visual axis, especially inferior ones, are a problem in a select group of people. These scars can be post-traumatic or post-infective. Because of such location, they interfere with visual function. Standard penetrating keratoplasty using allograft is the preferred procedure in majority of such cases.1-3 However, in a select group of patients, cornea can be rotated to change the location of the opacity. They have the advantage that they do not develop corneal graft rejection, which is an immune mediated response and which is the most common cause of graft failure after Penetrating Keratoplasty (PKP) using allograft.4 The purpose of this report is to document a corneal autograft where a completely opaque cornea of a patient was swapped with the clear cornea from the opposite eye.
Case Report
A 40-year-old-man presented to the eye clinic of Aga Khan University, Karachi with decreasing vision in the right eye. Both eyes were injured as a result of a bomb blast injury in late 2001. At that stage the vision was perception of light in the right and hand movements in the left eye. He underwent vitreo-retinal surgery for left retinal detachment in Jan 2002. Right corneal transplant with cataract extraction and lens implantation was performed in September 2002. Visual acuity remained poor even after these procedures.
He presented to our clinic in November 2009 with deteriorating vision in the right eye. On examination, his visual acuity was light perception in the right eye and no perception of light in the left. The right eye had an opaque cornea while the left eye had a clear one. Ultrasound examination of the right eye showed intact retina and clear vitreous cavity. The patient reported that he had been offered a corneal transplant in the right eye in another hospital he visited and he wanted a second opinion. Based on the findings - a left eye with clear cornea and no perception of light and right eye with opaque cornea and positive perception of light - we offered him a corneal auto-graft. The patient agreed. An 8 mm full thickness corneal button was removed from each eye and the left corneal button was grafted in the right eye and right opaque corneal button was grafted in the left eye (Figures-1 & 2).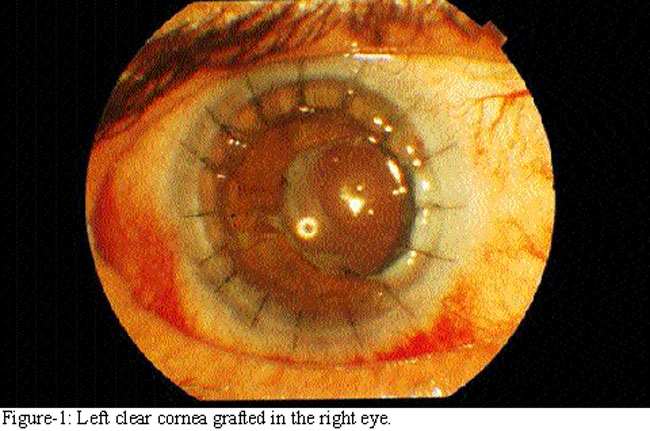

The patient was evaluated at 24 hours, 1 week and 1 month. At the 1 month, the best corrected visual acuity in the right improved from light perception to 20/400. The graft gave him navigational vision and the patient was satisfied with the visual outcome.
Discussion
To the best of our knowledge, this is the first report of corneal autograft in Pakistan. Corneal autografts are rare. Most of the reported cases involved rotation of the cornea in the same eye.4,5 After literature search it was determined that this is the first case in the country where a completely opaque cornea was swapped with a clear cornea from the opposite eye. Corneal autografts can be an option in injuries/situations where cornea in one eye is opaque with intact posterior segment while the cornea in the fellow eye is clear with severely damaged posterior segment. Given the increasing incidence of injuries in developing countries such as Pakistan a select group of individuals can benefit from this.The patient was able to achieve only navigational vision because of having a damaged posterior segment associated with bomb blast injury. The patient was satisfied with the visual outcome as he could function independently.
In routinely done corneal transplants, the risk of rejection is substantial because of the immune response leading to graft failure. The response is mediated by the cytotoxic T-cells of the immune system in response to antigens that are recognized as non-self by the body.
Conclusion
Corneal autograft in this case was successful and resulted in good navigational vision.
References
1.Cursiefen C, Kuchle M, Naumann GO. Changing indications for penetrating keratoplasty: histopathology of 1,250 corneal buttons. Cornea 1998; 17: 468-70.
2.Brady SE, Rapuano CJ, Arentsen JJ, Cohen EJ, Laibson PR. Clinical indications for and procedures associated with penetrating keratoplasty, 1983-1988. American journal of ophthalmology 1989; 108: 118-22.
3.Dobbins KR, Price FW Jr, Whitson WE. Trends in the indications for penetrating keratoplasty in the midwestern United States. Cornea 2000; 19: 813-6.
4.Rao SK, Lam DS. Calculating graft size and position in rotational corneal autografting: a simplified approach. Indian J Ophthalmol 2008; 56: 233-5.
5.Arnalich-Montiel F, Dart JK. Ipsilateral rotational autokeratoplasty: a review. Eye (Lond) 2009; 23: 1931-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: