
Syed Muhammad Baqir ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
Kiran Ejaz ( Department of Emergency Medicine, Aga Khan University Hospital, Karachi. )
December 2011, Volume 61, Issue 12
Editorial
Injury accounts for 16% of the global burden of disease. As one of the leading causes of mortality and morbidity worldwide, it overwhelmingly affects low and middle income countries.1,2 Evidence has shown that deaths are prevented and disability averted for conditions such as trauma, pregnancy, myocardial infarction, stroke and sepsis by upgrading the emergency services.3-5
Pre-hospital care research in developing countries has, to a large extent, focused on trauma. Mortality from severe injury occurs in one of the following three phases:
1) Immediate phase occurs as a result of overwhelming injury
2) Intermediate or sub-acute phase involves deaths occurring within several hours of the event and are potentially treatable.
3) Delayed phase when deaths often occur days or weeks after the initial injury.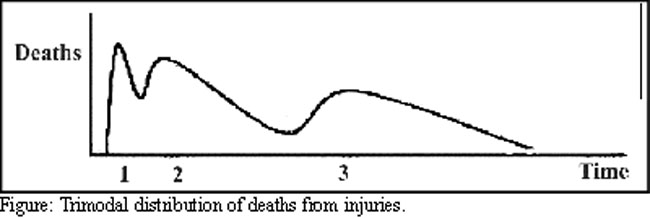
Figure illustrates this trimodal distribution of injury.2
The general understanding is that patients have better disease outcome if provided with definitive care within 60 minutes of the occurrence of injuries. Hence, pre-hospital care is most beneficial during the second phase of the conditions such as trauma. This timely provision of care can limit or halt the cascade of events that otherwise rapidly lead to death or lifelong disability. Without standard pre-hospital care, people with good survival possibilities also die at the scene or en route to the hospital. Most deaths in the early hours after injury are the result of airway compromise, respiratory failure or uncontrolled haemorrhage.6 All three of these conditions can be readily managed using basic first aid measures.
Similarly, in one study acute myocardial infarction patients receiving pre-hospital care had a lower in-hospital mortality compared to those first seen and managed in the hospital (8% vs 13%, P=<0.04).7 The American Heart Association has issued a scientific statement on the use of pre-hospital electrocardiograms to improve the quality of care delivered to patients with ST-segment-elevation myocardial infarction.8
There is a debate regarding how much care should be provided at the scene of incidents. Some are of the opinion that interventions may cause delay in the patient\\\'s arrival to a hospital and thus the patient should be transported without any treatment. Others favour teaching pre-hospital personnel skills to allow treatment to commence immediately after the event. The teaching must aim to strike a middle road to allow immediate care personnel to weigh the benefit of a particular skill against the possible detriment to the patient caused by the delay in transportation.9 This concept has been welcomed but is still considered novel as paramedics are generally taught to work using clearly defned protocols of different clinical scenarios, rather than making judgment decisions.
Emergency Medical Services (EMS) constitute both pre-hospital and hospital services. Both have long been neglected in many countries of the developing world.3,10 In Pakistan, few victims receive treatment at the scene and fewer still can hope to be transported to the hospital in an ambulance. Patients are instead brought to the Casualties/Emergency Departments (ED) by relatives or bystanders in private cars, taxis or any other readily available mode of transportation. Patients commuting to major cities from remote areas are most vulnerable. They often do not have any means of transportation and have to travel on foot without any first aid. In another study, the most common mode of transport to the Casualty/ED was found to be taxi (58%) followed by private car (23%).11 Specific reasons for not using ambulances included a perception that the patient was not sick enough (45%), slow response of the ambulance services (23%), not knowing how to find one (11%) and the high cost (8%). Hence, we can see that the reasons for this low usage include not only poor accessibility, but also cultural barriers and lack of education in recognition of danger signs.
In the metropolitan city of Karachi, ambulances, where they exist, have barely a comfortable gurney and arrangements for oxygen supply. As a result, the public does not perceive EMS as medical care providers. People view it only as transportation with sirens. Such vehicles do not reach the hospital earlier due to multiple reasons such as distance, traffic jams and poor public cooperation. Therefore many victims die a preventable death at the scene or during the first few hours following injury. Those making decisions at the critical moment on the site of the emergency are seldom aware of the factors one should keep in mind when taking affected person to a hospital.
Selection of a good ambulance service has a key role in the disease outcome of the patient. In Karachi, ambulance services have been evolving over the past few years. Earlier, ambulance services from St. John Association and Edhi Foundation played an active role, bearing the burden of the majority of such incidences.12,13 Lately, Chhipa and Aman Foundation have also joined the list.14,15 The City District Government Karachi Ambulance Service has been present but the change of administrations affects the continuity of services.16
Until the initiation of the Aman Foundation\\\'s EMS, no service existed in Karachi that provides advanced life support to victims on site.15 The majority of Karachi\\\'s ambulances are merely transport vehicles with untrained staff and little or no lifesaving equipment or supplies. Presence of facilities of paramedics with equipment for pre-hospital care can significantly lead to alteration in the disease outcomes and burden in the area. However, since the cost of an ambulance service varies depending on the type of ambulance and the distance to be covered, it often proves to be very expensive for a large percentage of Karachi\\\'s population. In addition, the location of ambulance stations in the city is haphazard and has little correlation with population density figures.
Edhi Foundation has tried to train and upgrade its enthusiastic helpers but the vast cover area and limited man power has affected its productivity. This is not to deny that the Edhi Foundation has raised the largest single fleet of ambulances in the country with an un-paralleled record of quick response for the victims of any disaster.13 Its nation-wide network equipped with the latest communication system now covers the remotest areas of Pakistan. A fleet of over four hundred ambulances, field mobile units and rescue units are maintained in a state of readiness to meet any emergency in the shortest possible time anywhere in Pakistan.
The evolution of ambulance services has lead to introduction of quality indicators in these services in the local setting. Among the systematic and clinical quality indicators, prompt response, availability of life saving drugs and oxygen, equipment such as intravenous catheters, electrocardiogram and glucometers are important. Training and education of the ambulance personnel including continuous training in advance life support is important.17
Cost is one aspect which cannot be ignored. The cost of running such services is high which has to be paid by the consumer. The challenge is to promote sustainable and affordable pre-hospital care systems that provide services to everyone. To do this, each system must be defined by local needs and capacity and must be developed according to local culture and health-care capacity. As a good example, "Rescue 1122" has managed to set up a low cost, effective system of pre-hospital care in Punjab, which can be replicated in other developing countries with little or no modification.18 Almost all the recommendations of the World Health Organization guidelines for pre-hospital trauma care systems have been fulfilled by them.2 However, prospective and retrospective clinical trials are needed to verify the efficacy of the system.
Like many other areas, we cannot depend upon public sector. Through self-help we, the healthcare personnel, need to find economical solutions for the betterment of our patients. One can easily understand the problems a non-affording citizen of a developing country has to face and accordingly make the selection of the ambulance services. We need to educate our masses regarding the importance of ambulances and pre-hospital care. Our people should be able to judge the characteristics and attributes of an effective ambulance service.
Disclaimer:
The authors do not favour or recommend any specific ambulance service.
References
1.Mock C, Lormand J, Gossen J, Joshipura M, Peden M. Guidelines for essential trauma care. Geneva: World Health Organization; 2004. (Online) 2004 (Cited 2011 September 23). Available from URL: http://whqlibdoc.who.int/ publications/2004/9241546409.pdf.
2.Sasser S, Varghese M, Kellermann A, Lormand J. Prehospital trauma care systems. Geneva: World Health Organization; 2005. (Online) 2005 (Cited 2011 September 15). Available from URL: http://whqlibdoc.who.int/publications/ 2005/924159294x.pdf.
3.Razzak JA, Kellermann AL. Emergency medical care in developing countries: is it worthwhile? Bull World Health Organ. 2002; 80: 900-5.
4.Mock CN, Adzotor KE, Conklin E, Denno DM, Jurkovich GJ. Trauma outcomes in the rural developing world: comparison with an urban level I trauma center. J Trauma 1993; 35: 518-23.
5.London JA, Mock CN, Quansah RE, Abantanga FA, Jurkovich GJ. Priorities for improving hospital-based trauma care in an African city. J Trauma 2001; 51: 747-53.
6.Scott S, Mathew V, Manjul J, Arthur K. Preventing death and disability through the timely provision of prehospital trauma care. Bulletin of the World Health Organization 2006; 84: 505-88.
7.Mathew TP, Menown IB, McCarty D, Gracey H, Hill L, Adgey AA. Impact of pre-hospital care in patients with acute myocardial infarction compared with those first managed in-hospital. Eur Heart J 2003; 24: 161-71.
8.O\\\'Riordan M, Lie D. AHA Publishes Statement on Integrating Prehospital ECGs Into Care for ACS Patients 2008. (Online) 2008 (Cited 2011 September 23). Available from URL: http://www.medscape.org/viewarticle/579069.
9.Cooke MW. How much to do at the accident scene? Spend time on essentials, save lives. BMJ 1999; 319: 1150.
10.Shah MN. The formation of the emergency medical services system.Am J Public Health 2006; 96: 414-23.
11.Razzak JA, Cone DC, Rehmani R. Emergency medical services and cultural determinants of an emergency in Karachi, Pakistan. PrehospEmerg Care 2001; 5: 312-6.
12.St. John. Too. St John Association of Pakistan 2004. (Online) 2004 (Cited 2011 September 23). Available from URL: http://www.orderofstjohn.org/pakistan.
13.Edhi Foundation. Edhi Foundation Services.Field Ambulance Services 2010. (Online) 2010 (Cited 2011 September 23). Available from URL: http://www.edhifoundation.com/edhi-foundation-services.asp#06.
14.Chhipa Welfare Association. CWA\\\'s 24 Hours Services at a glance 2007. (Online) 2007 (Cited 2011 September 23). Available from URL: http://www.chhipa.org/services.php.
15.Aman Foundation. Aman Health 2011. (Online) 2011 (Cited 2011 September 23). Available from URL: http://www.amanfoundation.org/projects/healthcare/.
16.City District Government Karachi. Health Department 2010. (Online) 2010 (Cited 2011 September 23). Available from URL: http://www.karachicity.gov.pk/.
17.Department of Health. Ambulance Quality Indicators 2011. (Online) 2011 (Cited 2011 September 23). Available from URL: http://www.dh.gov.uk/en/Publicationsandstatistics/Statistics/Performancedataandstatistics/AmbulanceQualityIndicators/index.htm.
18.Waseem H, Naseer R, Razzak JA. Establishing a successful pre-hospital emergency service in a developing country: experience from Rescue 1122 service in Pakistan. Emerg Med J 2010; 28: 513-5.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: