
Syed Haider Imam ( Medical College, Section of Cardiology, Aga Khan University Hospital, Karachi, Pakistan. )
Abbas Haider Zaidi ( Medical College, Section of Cardiology, Aga Khan University Hospital, Karachi, Pakistan. )
Sana Shoukat ( Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan. )
Sajid Hamid Dhakam ( Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan. )
November 2011, Volume 61, Issue 11
Student's Corner
Abstract
This study evaluated the short and long-term consequences of Percutaneous Mitral Valvuloplasty (PMV) in pregnant patients and their offspring, in a tertiary care setting, Karachi, Pakistan.
The hospital database was used to retrieve all patients who underwent PMV during pregnancy in the period 1998- 2007. The follow up data of the patients and the born children were obtained from the hospital records and also by contacting the patients via phone.
Six patients underwent PMV but follow-up was available for 5 patients only. All 5 patients were admitted due to severe mitral stenosis with symptoms of dyspnea and palpitation. Mean age was 27 ± 5.3 years with a mean gestational age at the time of procedure of 22.20 ± 1.6 weeks. The mean valve area increased from 0.94 ± 0.22 cm2 pre-operatively to 1.62 ± 0.50 cm2 post-operatively. The ejection fraction changed from a mean of 50 ± 11.7 % to 56 ± 2.2 %. There were no maternal deaths, abortions or stillbirths. Developmental milestones were achieved at the appropriate ages in all babies.
PMV appears to be a safe and effective intervention for patients with severe MS during pregnancy.
Keywords: Mitral stenosis, Percutaneous Mitral valvuloplasty, Pregnancy.
Introduction
Mitral stenosis (MS) is the most common valvular lesion seen in pregnancy worldwide and is often the most poorly tolerated.1 Problems associated with mitral stenosis in pregnancy are due to further narrowing of mitral valve and the haemodynamic change that take place.2 Pregnancy is a burden even in normal patients by causing an increase of 30% to 50% in intravascular volume. This can lead to an increase in transmitral gradient and left atrial pressure and also cause flash pulmonary oedema.3 Maternal mortality for patients with MS are significantly higher (6.8%) for those who are New York Heart Association (NYHA) class 3 and 4 than patients who are NYHA class 1 and 2 (0.4%), particularly during labour and delivery.4
These symptoms usually become apparent by the 20th week of pregnancy and can be aggravated even further at the time of labour and delivery. Maternal death is rare when careful attention is paid to the management of congestive heart failure.5 Percutaneous Mitral valvuloplasty (PMV) is indicated in symptomatic patients with mitral stenosis.2,6 For pregnant patients, however, medical management is recommended and PMV only if the patient fails medical management during pregnancy with repetitive or persistent heart failure. There exists more than ten years experience with PMV in pregnant patients in the literature.7 However, the safety and efficacy of this procedure has not been clearly established for pregnant patients. Surgical commissurotomy is indeed effective but with higher maternal mortality rate (1.7%-3.1%) and infant mortality rate ranging from 5% to 33%.4,8
In our part of the world, MS is the major lesion found during pregnancy, the main cause of which is rheumatic heart disease.9,10 This is attributed to poor socio-economic status, overcrowded living conditions and poor access to medical care.9 The data from Pakistan is scarce, and to our knowledge few studies have been done regarding the effects of PMV on pregnancy outcome and the newborn child.
The objective of this study was to evaluate short and long-term consequences of PMV, in a tertiary care setting, Karachi, Pakistan.
Methods
The Aga Khan University Hospital database was used to retrieve all patients who underwent PMV during pregnancy between the period of 1998 and 2007. The follow up data of the patients and the born children were obtained from the medical records available and follow up was done by contacting the patients via phone.
All pregnant women presenting with mitral valve disease (Mitral stenosis and regurgitation) and undergoing PMV from 1998-2007 were included in this study. Patients who were not available for follow-up were excluded from the study.
Patients were followed up to document residual symptoms of mitral valve disease (NYHA class), procedure-related complications, need for surgical intervention post-PMV. Possible maternal confounding factors such as co-morbidities were also documented. Pregnancy outcomes such as weight of the new-born, CTG (cardiotocography), mode and complications of delivery, post-natal well-being as well as developmental milestones or delays were also recorded.
A baseline echocardiogram was performed in all patients. PMV was performed after taking an informed written consent as per standard protocol. Antibiotic prophylaxis was initiated in all patients thereafter. The procedure was performed under local anaesthesia and lead abdominal protection was used in all patients.
Summary statistics are presented using mean and standard deviation (mean ± SD) for continuous variables and using frequencies for categorical variables.
Results
From 1998 to 2007, a total of 56 patients underwent PMV at the Aga Khan University Hospital, Karachi, Pakistan. Out of the 39 females, 6 were pregnant and had mitral stenosis for which they had mitral valvuloplasty done. Follow-up for 5 patients was available as there was a loss to follow up of 1 patient. Average follow-up for this study was 4.5 years conducted in March 2009. These five women were admitted due to severe mitral stenosis with common presentation of dyspnoea and palpitations. Other symptoms included exertional chest pain, productive cough and atrial fibrillation. One of the patients also had a history of atrial septal defect. The mean age of patients was 27.0 ± 5.3 years, with a mean gestational age at the time of procedure of 22.2 ± 1.6 weeks.
Follow-up of the infant after birth was also available for all five patients and is presented in Table-1.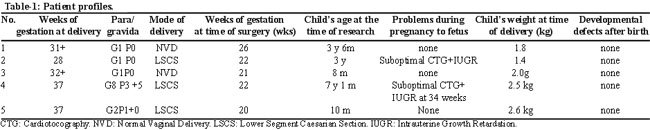
There was a noteworthy increase in valve area and decrease in mean pressure gradient (MPG) after PMV (Table-2).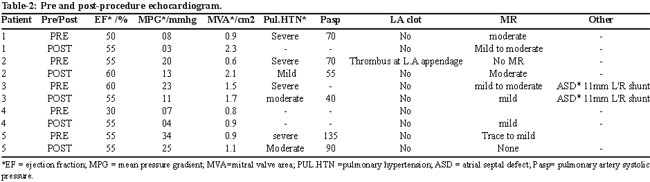
The mean valve area increased from 0.94 ± 0.22 cm2 pre-operatively to 1.62 ± 0.50 cm2 post-operatively. The ejection fraction changed mildly from a mean of 50 ± 11.7% to 56 ± 2.2%.
Only one patient had atrial fibrillation and hypertension post-procedure. Most patients did not show any recurrence of symptoms or any problem related to previously diagnosed mitral stenosis after the valvuloplasty and there was improvement in NYHA class of heart failure in all patients (Table-3).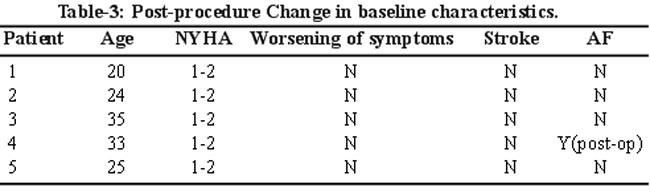
One patient had to undergo mitral valve replacement after one year due to persistent symptoms (chest pain and dyspnoea). Two patients had infant birth through normal vaginal delivery while the other three had them through Caesarean section. There were no maternal deaths, abortion or stillbirths seen. Two patients delivered prematurely and Intrauterine growth retardation with sub-optimal Cardiotocography (CTG) were seen in their foetuses (50%). The infants were born with a mean weight of 2.1 ± 0.50 kg. These infants were followed up till July 2007 over a period of average 158 weeks. Their mean age was 36.2 ± 5.9 months. All babies were normal at birth and maintained normal growth and development without any thyroid disease or malignancy. Developmental milestones were achieved at the appropriate ages in all babies.
Discussion
PMV has largely replaced surgical valvulotomy or MVR in MS in the absence of contraindications11 and newer approaches to valve replacement are being carried out.12 The aim of PMV during pregnancy is to relieve symptoms and prevent adverse effects on foetal well being due to the haemodynamic compromise. In Pakistan where antenatal diagnosis of MS is frequently missed,13 this becomes a very important tool to help mother and baby during pregnancy but the adverse effects and potential complications associated with the procedure has always been a concern to the health of mother and infant alike, especially due to the use of contrast and radiation during the procedure.14,15 This radiation can have potential teratogenic effects. The nature and severity of the harmful effects to the embryo or foetus associated with radiation are related to the gestational age at which the exposure occurs.16 Fatal effects include organ malformation, severe mental retardation and malignancy, especially leukaemia.17,18
Our findings are consistent with other data in which the major symptoms, gestational age at the time of procedure, outcomes of pregnancy and long-term follow up closely correlate with our patients.7,19,20 However, the percentage of pre-term delivery was higher in our series, which is likely because of the small sample size and were not seen in other studies.21 No abnormalities in growth or development were seen. Two cases of premature delivery were seen leading to a procedure. This caused us to speculate that this might be related to the effects of either mitral stenosis during pregnancy and its effects on the foetus or due to mitral valvuloplasty and the radiation being used.22-24 However, there is no reported case of abortion or still birth in our study. Although still birth and abortion rates are very low, they were present in other studies.19,24 The functional class improved dramatically to NYHA class 1 or 2 which is again consistent with other studies in literature.7,19,20
Although certain protective measures were carried out during the procedures in our study, including the use of abdominal shield and the procedure being done only in women over 20 weeks of gestation, there was still a further need to investigate and follow-up the mothers and the infants to identify any long term side effects of this procedure.
Our study is a small observation especially in terms of long-term follow-up of patients who required PMV and long-term follow-up of their children. Though it is difficult to draw conclusions due to the small sample size but our observation shows that PMV is a relatively safe procedure, both for the mother and the child even after a long-term follow-up like an average of 4.5 years (234 weeks) in our study.
In summary, for pregnant patients who have severe mitral stenosis and persistent heart failure along with pulmonary hypertension, mitral valvuloplasty is a safe, feasible and effective treatment with no obvious long-term complications for both mother and foetus.2,5,7,18-21,24
Conclusion
PMV appears to be a safe and effective intervention for patients with severe MS during pregnancy. Larger definitive studies, however, need to be executed especially in our population.
References
1.Lin JH, Ling WW, Liang AJ. [Pregnancy outcome in women with rheumatic heart disease]. Zhonghua Fu Chan Ke Za Zhi 2007; 42: 315-9.
2.Weiss BM. Managing severe mitral valve stenosis in pregnant patients--percutaneous balloon valvuloplasty, not surgery, is the treatment of choice. J Cardiothorac Vasc Anesth 2005; 19: 277-8.
3.Nobuyoshi M, Arita T, Shirai S, Hamasaki N, Yokoi H, Iwabuchi M, et al. Percutaneous balloon mitral valvuloplasty: a review. Circulation 2009; 119: e211-9.
4.de Souza JA, Martinez EE Jr, Ambrose JA, Alves CM, Born D, Buffolo E, et al. Percutaneous balloon mitral valvuloplasty in comparison with open mitral valve commissurotomy for mitral stenosis during pregnancy. J Am Coll Cardiol 2001; 37: 900-3.
5.Moghbeli N, Pare E, Webb G. Practical assessment of maternal cardiovascular risk in pregnancy. Congenit Heart Dis 2008; 3: 308-16.
6.Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008; 118: e523-661.
7.Esteves CA, Munoz JS, Braga S, Andrade J, Meneghelo Z, Gomes N, et al. Immediate and long-term follow-up of percutaneous balloon mitral valvuloplasty in pregnant patients with rheumatic mitral stenosis. Am J Cardiol 2006; 98: 812-6.
8.Elkayam U, Bitar F. Valvular heart disease and pregnancy part I: native valves. J Am Coll Cardiol 2005; 46: 223-30.
9.Asghar F, Kokab H. Evaluation and outcome of pregnancy complicated by heart disease. J Pak Med Assoc 2005; 55: 416-9.
10.Rizvi SF, Khan MA, Kundi A, Marsh DR, Samad A, Pasha O. Status of rheumatic heart disease in rural Pakistan. Heart 2004; 90: 394-9.
11.Vahanian A, Acar C. Percutaneous valve procedures: what is the future? Curr Opin Cardiol 2005; 20: 100-6.
12.Feldman T, Herrmann HC, St Goar F. Percutaneous treatment of valvular heart disease: catheter-based aortic valve replacement and mitral valve repair therapies. Am J Geriatr Cardiol 2006; 15: 291-301.
13.Bhutta SZ, Aziz S, Korejo R. Pregnancy following cardiac surgery. J Pak Med Assoc 2003; 53: 407-13.
14.Safian RD, Berman AD, Sachs B, Diver DJ, Come PC, Baim DS, et al. Percutaneous balloon mitral valvuloplasty in a pregnant woman with mitral stenosis. Cathet Cardiovasc Diagn 1988; 15: 103-8.
15.Cheng TO. Long-term results of percutaneous balloon mitral valvuloplasty using the Inoue balloon catheter technique. Circulation 2000; 101: E91.
16.Mangione JA, Lourenco RM, dos Santos ES, Shigueyuki A, Mauro MF, Cristovao SA, et al. Long-term follow-up of pregnant women after percutaneous mitral valvuloplasty. Catheter Cardiovasc Interv 2000; 50: 413-7.
17.Fattibene P, Mazzei F, Nuccetelli C, Risica S. Prenatal exposure to ionizing radiation: sources, effects and regulatory aspects. Acta Paediatr 1999; 88: 693-702.
18.Balter S. Radiation safety in the cardiac catheterization laboratory: operational radiation safety. Catheter Cardiovasc Interv 1999; 47: 347-53.
19.Sivadasanpillai H, Srinivasan A, Sivasubramoniam S, Mahadevan KK, Kumar A, Titus T, et al. Long-term outcome of patients undergoing balloon mitral valvotomy in pregnancy. Am J Cardiol 2005; 95: 1504-6.
20.Salome N, Dias CC, Ribeiro J, Goncalves M, Fonseca C, Ribeiro VG. Balloon mitral valvuloplasty during pregnancy - our experience. Rev Port Cardiol 2002; 21: 1437-44.
21.Routray SN, Mishra TK, Swain S, Patnaik UK, Behera M. Balloon mitral valvuloplasty during pregnancy. Int J Gynaecol Obstet 2004; 85: 18-23.
22.Chohan U, Afshan G, Mone A. Anaesthesia for caesarean section in patients with cardiac disease. J Pak Med Assoc 2006; 56: 32-8.
23.Hameed A, Karaalp IS, Tummala PP, Wani OR, Canetti M, Akhter MW, et al. The effect of valvular heart disease on maternal and fetal outcome of pregnancy. J Am Coll Cardiol 2001; 37: 893-9.
24.Nercolini DC, da Rocha Loures Bueno R, Eduardo Guerios E, Tarastchuk JC, Pacheco AL, Pia de Andrade PM, et al. Percutaneous mitral balloon valvuloplasty in pregnant women with mitral stenosis. Catheter Cardiovasc Interv 2002; 57: 318-22.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: