
Hamid Majeed ( Department of Radiology, Sharif Medical & Dental College, Lahore. )
Amaila Ramzan ( Department of Radiology, Shoukat Khanum Cancer Hospital & Research Centre, Lahore. )
Faiqa Imran ( Department of Gynaecology & Obstetrics, Central Park Medical College, Lahore. )
Mahfooz-ur-Rehman ( Department of Radiology, Sharif Medical & Dental College, Lahore. )
November 2011, Volume 61, Issue 11
Original Article
Abstract
Objective: To evaluate the validity of resistive index (RI) in conjunction to the morphological appearances.
Methods: Prospective cross sectional survey of 37 females with adnexal masses was selected through non probability sampling admitted in Obstetrics units, in a private hospital from January 2009 to March 2010. All women underwent transabdominal and transvaginal ultrasound and ovarian masses were characterized as probably benign or possibly malignant on the basis of their sonographic appearance. The RI was calculated in every case and threshold RI of 0.40 was used to differentiate benign from malignant lesions. Later pathologic proof was obtained in every case. Validity of the RI was calculated considering the histopathology as gold standard.
Results: Out of these 37 masses, 19 were morphologically benign and pathology revealed the same results. The RI was less than 0.4 in 3 of these cases. Eighteen lesions were morphologically either malignant (or indeterminate). On pathologic examination, 7 were benign, 2 were nonneoplastic masses, and 9 were malignant neoplasm. The RI was greater than 0.4 in 8 of these cases and was less than 0.4 in only 2 of the eight lesions. Sensitivity of the RI was 18.18% in diagnosing the malignancy whereas the specificity was only 84.61%. Positive predictive value of RI to differentiate benign from malignant lesions was only 33.33% and negative predictive value was 70.96%. Thus the accuracy of the RI was 64.86% with precision of only 33.33%.
Conclusion: Resistive index may improve specificity in characterizing malignant ovarian lesions on ultrasound, but it can be misleading.
Keywords: Ultrasonography, Resistive index, Malignant, Adnexal masses (JPMA 61: 1104; 2011).
Introduction
Ultrasonography (US) is accepted as a valuable imaging modality in the evaluation of an ovarian mass.1 The use of US in the detection of a suspected ovarian mass and in its differentiation from a uterine mass has been well established. As, US depict the mass, characterization of the mass is typically performed during the same examination.
A majority of ovarian masses are nonneoplastic cysts. However, when a lesion is suspected of being a neoplasm, surgical intervention must be considered. Twenty-five percent of ovarian neoplasms are malignant.2 For this reason, surgical removal of a suspected ovarian neoplasm is the standard procedure. In most institutions, the type of surgery performed (laparoscopy vs laparotomy) depends on the probability of malignancy. The optimal US technique and diagnostic criteria to use when characterizing a suspected ovarian neoplasm remain controversial. The reported accuracy of US is 65%-94%3,4 for gray-scale US, 35%-88%5,6 for colour Doppler flow imaging, and 48%-99%3,7 for Doppler arterial resistance measurements. In addition, diagnostic algorithms and multiparameter scoring systems have been advocated to increase test performance.8-10 The question of which US technique and diagnostic criteria provide the best ovarian lesion characterization has not, to our knowledge, been answered. Transvaginal sonography has been advocated as a screening method for ovarian cancer because masses can be detected by this technique before they are clinically apparent.2,4 Current research also suggests that determining the resistance of blood flow in and around adnexal masses is a sensitive method for detecting ovarian cancer and that benign lesions can be differentiated from malignant ovarian masses on the basis of the resistive index (RI).5,7 In the largest reported series, the sensitivity was 99.7% and the specificity was 96.4% when an RI of 0.4 on less was used to classify lesions as malignant.7
The sonographic features of benign and malignant adnexal masses have been well described.11 Scoring methods have been developed with sensitivities up to 100% for differentiating benign from malignant lesions.12
Criteria for benign lesions include an anechoic lesion with a thin smooth wall and no septations. Other benign masses may have a characteristic appearance. One such lesion is the endometriotic cyst, which has diffuse low-level echoes with or without a few thin septations. Another is the dermoid cyst, which has a fluid layer or an echogenic mural nodule with shadowing. Features that suggest malignancy include irregularities in the wall of the mass, thick septations, and solid components. It has been our experience that the RI often contradicts our morphologic assessment of lesions as benign on malignant. We devised a study to compare the sensitivity and specificity of morphologic findings on sonograms and the RI for differentiating benign from malignant adnexal masses.
Patients and Methods
Between July 01, 2009 and July 01, 2010, 37 women, 17-74 years old (mean age 36.21±15.8 years) who underwent pelvic sonographic evaluation of an adnexal mass with gray-scale and Doppler examinations and who later had surgical removal of the lesion were included in the study. Patients were identified for the study at the time of initial sonographic evaluation. Twenty-six were premenopausal, nine were postmenopausal, and two were perimenopausal. The indication for sonography was evaluation of a pelvic mass in 17, pain in 9, Dysfunctional uterine bleeding in 4 and seven women underwent routine screening.
A total of 37 masses were examined transabdominally with a 3.5-MHz transducer and transvaginally with a 5-MHz transducer with Doppier capability. All sonograms were obtained with Hitachi 5500. Color Doppler imaging was used to guide placement of the Doppler gate for pulsed Doppler analysis. RI (RI = [peak systolic velocity - end diastolic velocity]/peak systolic velocity) was calculated for any vessel at the periphery or within the mass. Sonograms were evaluated by two experienced sonologists. The size, echogenicity, wall thickness, and presence of septations and endocystic vegetations were determined for each mass. The lesions were classified as benign, indeterminate, or malignant. Morphologically, benign lesions had the classic appearance of a simple cyst (anechoic with a thin wall and acoustic enhancement, with or without a single thin septation), a dermoid (cyst with fluid layer or echogenic mural nodule with shadowing), or an endometrioma (cyst with diffuse low-level echoes with one or two thin septations and a thin wall. Indeterminate lesions had a predominantly benign appearance with atypical features such as a thick wall or thick, multiple, or irregular septations (Fig. 1). Morphologically malignant lesions had nodules or solid elements. For statistical purposes, lesions deemed indeterminate and malignant were grouped together as possibly malignant. Surgical pathologic reports for 37 lesions were reviewed. SPSS version 17 was used to configure the data.
Results
Twenty-six lesions were benign and eleven were malignant on pathologic examination. Benign lesions included fifteen chocolate cysts or endometriomas, five cystadenomas, two mature teratomas and four were simple follicular cysts. Histologically, malignant lesions included four serous papillary carcinomas, two granulosa cell tumors, two cystadenocarcinomas and one metastasis from gastric primary.
The mean of the lowest recorded RI for the benign lesions was 0.56 ± 0.14 (range, 0.32-0.8). The mean lowest RI for malignant lesions was 0.52 ± 0.11 (range, 0.35-0.7). Nineteen lesions were morphologically benign on sonograms and pathology revealed all these to be benign. The RI was greater than 0.4 in 15 of these 1 9 cases. Three endometriomas had low RIs of 0.32, 0.36, and 0.37. Eight lesions could not be characterized properly and were considered as indeterminate lesions. Histopathology, revealed that 5, out of these 8 lesions, were endometriomas, and 2 were cystadenomas and one was a cystic granulosa cell tumour. The RI was greater than 0.4 in six of the seven that were benign and in the granulosa cell tumour. The RI was 0.32 in one endometrioma. Ten lesions were characterized as malignant on the basis of sonographic features. Pathologic examination showed that eight of the 10 were malignant. The other two were ruptured cysts with haemorrhage and inflammation. The RI was less than 0.4 in two of the eight malignant lesions with malignant morphology. It was greater than 0.4 in the other seven malignant and two benign lesions in this category (Figure-1&2).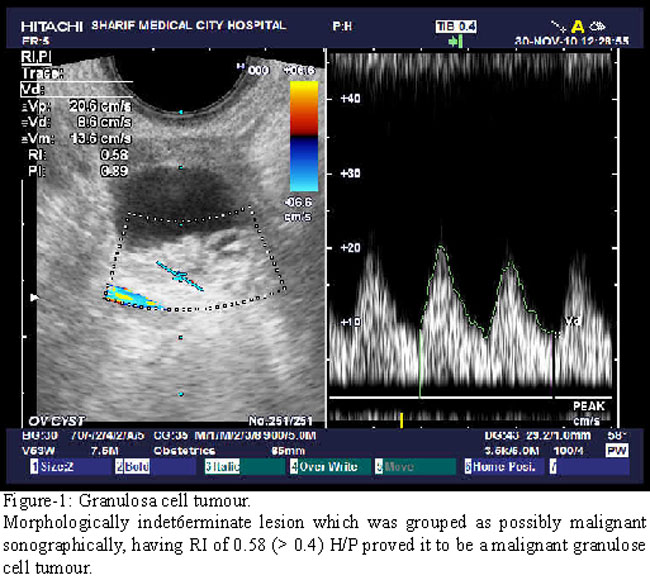

Combining the lesions deemed indeterminate and malignant on the basis of sonographic features, 18 lesions were characterized as possibly malignant. Pathologic examination showed that nine of these lesions were actually malignant. The RI was less than 0.4 in only two of these neoplasms (Figure-3).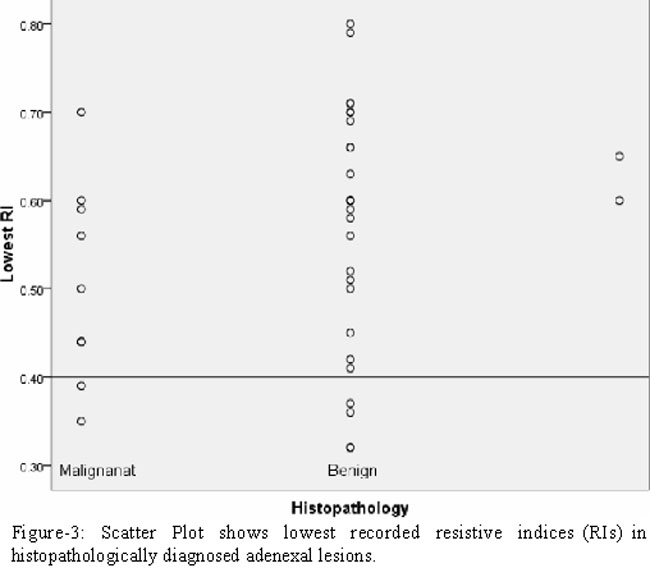
When checking the validity of the resistive index sensitivity turned out to be 18.18% in diagnosing the malignancy while the specificity was 84.61%. Positive predictive value of resistive index to distinguish benign from malignant tumours was merely 33.33% and negative predictive value was 70.96%. As a result the accuracy of the resistive index was 64.86% with Precision of just 33.33% (Figure-4).
Discussion
The preoperative imaging characterization of an ovarian mass directly affects surgical decisions and subspecialty referral and is therefore important for patient treatment. Although gray-scale US remains a mainstay of imaging detection of suspected ovarian masses, persisting controversies surround the optimal US techniques for subsequent characterization of the detected ovarian mass.13
Most adnexal masses detected with sonography are physiologic cysts, for which surgery is not indicated. We intentionally excluded physiologic cysts, such as corpus luteal cysts, as they may have a low RI14,15 that would have decreased the specificity of our RI measurements. The purpose was to assess whether the RI has any place in the evaluation of masses for which surgery is indicated. When such an adnexal mass is detected, information about the likelihood that the mass is benign or malignant is important, because this will affect the clinical management and possibly the surgical approach. For this reason, we grouped our sonographic impressions as probably benign and possibly malignant. With strict application of morphologic criteria, all nine malignant lesions were correctly categorized as possibly malignant. This gave gray-scale sonography a sensitivity of 100% for the diagnosis of malignant disease. However, pathologic examination showed that two of 11 lesions classified as malignant on the basis of morphology and seven of eight lesions with indeterminate morphology were benign, yielding a specificity of more than 60% for sonography. We accepted a lower specificity for sonography in order to achieve a high sensitivity and not miscategorize malignant lesions. We approached lesions with possibly malignant morphology as malignant until proved otherwise. However, the RI would be helpful in the assessment of indeterminate lesions if it could increase specificity without decreasing sensitivity. Among the lesions classified as indeterminate on the basis of sonographic findings, the RI was greater than 0.4 in the sole malignant lesion; thus, use of this parameter was not helpful. When a threshold of 0.4 was used for the 37 lesions in the study, the sensitivity of the RI was 18.18% and the specificity was 84.61% for detection of malignant lesions. Significantly, six of eight neoplasms were incorrectly characterized as benign on the basis of their RIs.
Our results are similar to those of other recent reports which show a sensitivity of 26-37% when a threshold RI of 0.4 or less is used.16-18 These articles emphasize that although vessels with low-resistance flow suggest a malignant lesion, some benign tumours (e.g., inflammatory masses and endometriomas) show this pattern. Likewise, malignant tumours frequently show high-resistance flow.
As in other studies, we used the lowest RI values for statistical analysis in order to detect the most suspicious areas in a neoplasm. Even when these lowest values were used, we found no significant difference between the RI of benign and malignant masses. Additionally, we found a significant variability in the RIs within individual masses. This is a potential problem when Doppler sonography is used. A recording from a single high-resistance vessel is not sufficient. A thorough search for other areas of flow must be performed to ensure that the lowest value is obtained. We recognize that sonography is sensitive but not specific for distinguishing between benign and malignant ovarian neoplasms.
Conclusion
Although use of RIs can improve specificity in the assessment of lesions considered possibly malignant morphologically, reliance on RIs is potentially misleading. On the basis of our results, the use of Doppler waveform analysis for determining whether an adnexal mass is benign or malignant is experimental at best and should be discouraged in clinical decision making.
References
1.Yazbek J, Helmy S, Ben-Nagi J, Holland T, Sawyer E, Jurkovic D. Value of preoperative ultrasound examination in the selection of women with adnexal masses for laparoscopic surgery. Ultrasound Obstet Gynecol 2007; 30: 883-8.
2.Koonings PP, Campbell K, Mishell DR, Jr, Grimes DA. Relative frequency of primary ovarian neoplasms: a 10-year review. Obstet Gynecol 1989; 74: 921-6.
3.Kurjak A, Predanic M. New scoring system for prediction of ovarian malignancy based on transvaginal color Doppler sonography. J Ultrasound Med 1992; 11: 631-8.
4.Salem S, White LM, Lai J. Doppler sonography of adnexal masses: the predictive value of the pulsatility index in benign and malignant disease. AJR Am J Roentgenol 1994; 163: 1147-50.
5.Tailor A, Jurkovic D, Bourne TH, Natucci M, Collins WP, Campbell S. A comparison of intratumoural indices of blood flow velocity and impedance for the diagnosis of ovarian cancer. Ultrasound Med Biol 1996; 22: 837-43.
6.Juhasz B, Kurjak A, Lampe L, Zalud I, Crvenkovic G, Hernadi Z. Tissue characterization by transvaginal colour Doppler for the evaluation of gynaecological tumours. 2. Clinical experiences. Acta Med Hung 1990; 47: 149-56.
7.Valentin L. Gray scale sonography, subjective evaluation of the color Doppler image and measurement of blood flow velocity for distinguishing benign and malignant tumors of suspected adnexal origin. Eur J Obstet Gynecol Reprod Biol 1997; 72: 63-72.
8.Bromley B, Goodman H, Benacerraf BR. Comparison between sonographic morphology and Doppler waveform for the diagnosis of ovarian malignancy. Obstet Gynecol 1994; 83: 434-7.
9.Brown DL, Doubilet PM, Miller FH, Frates MC, Laing FC, DiSalvo DN, et al. Benign and malignant ovarian masses: selection of the most discriminating gray-scale and Doppler sonographic features. Radiology 1998; 208: 103-10.
10.Alcazar JL, Jurado M. Using a logistic model to predict malignancy of adnexal masses based on menopausal status, ultrasound morphology, and color Doppler findings. Gynecol Oncol 1998; 69: 146-50.
11.Granberg S, Wikland M, Jansson I. Macroscopic characterization of ovarian tumors and the relation to the histological diagnosis: criteria to be used for ultrasound evaluation. Gynecol Oncol 1989; 35: 139-44.
12.Sassone AM, Timor-Tnitsch IE, Artner A, Westhoff C, Warren WB. Transvaginal sonographic characterization of ovarian disease: evaluation of a new scoring system to predict ovarian malignancy. Obstet Gynecol 1991; 78: 70-6.
13.Greenlee RT, Kessel B, William CR, Riley TL, Ragard LR, Hartge P, et al. Prevalence, incidence, and natural history of simple ovarian cysts among women > 55 years old in a large cancer screening trial. Am J Obstet Gynecol 2010; 202: 373.e1-9.
14.Hamper UM, Sheth 5, Abbas FM, Rosenshein NB, Aronson D, Kurman AJ. Transvaginal color Doppler sonography of adnexal masses: differences in blood flow impedance in benign and malignant lesions. Am J Roentgenol 1993; 160: 1225-8.
15.Timor-Tnitsch IE, Lerner JP, Monteagudo A, Santos A. Transvaginal ultrasonographic characterization of ovarian masses by means of color flowdirected Doppler measurements and a morphologic scoring system. Am J Obstet Gynecol 1993; 168: 909-13.
16.Parker WH. Management of adnexal masses by operative laparoscopy. Selection criteria. J Reprod Med 1992; 37: 603-6.
17.Schneider VL, Schneider A, Reed KL, Hatch KD. Comparison of Doppler with two-dimensional sonography and CA 125 for prediction of malignancy of pelvic masses. Obstet Gynecol 1993; 81: 983-8.
18.Hata K, Hata T, Manabe A, Sugimura K, Manabu K. A critical evaluation of transvaginal Doppler studies, transvaginal sonography, magnetic resonance imaging, and CA 125 in detecting ovarian cancer. Obstet Gynecol 1992; 80: 922-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: