
Azin Alizadehasl ( Cardiovascular Research Centre, Tabriz University of Medical Sciences, Tabriz, Iran. )
Zahra Golmohammadi ( Cardiovascular Research Centre, Tabriz University of Medical Sciences, Tabriz, Iran. )
Lale Panjavi ( Cardiovascular Research Centre, Tabriz University of Medical Sciences, Tabriz, Iran. )
Siamak Mahmoodmoradi ( Cardiovascular Research Centre, Tabriz University of Medical Sciences, Tabriz, Iran. )
Rasoul Azarfarin ( Cardiovascular Research Centre, Tabriz University of Medical Sciences, Tabriz, Iran. )
November 2011, Volume 61, Issue 11
Original Article
Abstract
Objective: To determine the frequency of anaemia in adult patients who were hospitalized with a diagnosis of cardiovascular disease in East Azerbaijan province, northwest Iran.
Methods: Overall 12031 adult patients with different cardiovascular disease (according to International Classification of Diseases vr. 10) were studied. These patients were hospitalized in 15 hospitals in East Azerbaijan province from March 2007 to March 2008. Patient\\\'s clinical characteristics were collected retrospectively, considering their main clinical diagnosis and co-morbidities and risk factors. Anaemia was defined as haemoglobin<12 g/dl in women and <13 g/dl in men based on WHO criteria.
Results: Among 12031 patients, 2913 (24.2%) were anaemic and 9118 were non-anaemic. The analysis of prevalence of anaemia showed that the highest proportion belonged to peripheral vascular disease with the prevalence rate of 56.1% followed by congenital heart disease (36.6%), heart failure (36.0%), valvular heart disease (34.0%) and pulmonary vascular disease (33.7%).There is a high rate of anaemia prevalence in age group older than 70 years and patients younger than 40 years. Multivariate logistic regression analysis revealed, being non-smoker, history of cardiac surgery, lower ejection fraction (<40%) and serum creatinin level > 1.2 mg/dl as independent predictors of anaemia.
Conclusion: Overall 24% of our cardiovascular disease patients had anaemia. Anaemia was more common among patients with peripheral vascular disease, then congenital heart disease and congestive heart failure. History of surgery, non-smoking, lower ejection fraction and higher serum creatinine level increase the incidence of anaemia.
Keywords: Anaemia, Cardiovascular diseases, Hospitalization, Congestive heart failure, Azerbaijan, Peripheral vascular disease (JPMA 61: 1091; 2011).
Introduction
Considering high prevalence of anaemia, interrelation with comorbidities, and direct impact on patient health, it has become a focus of clinical and research interest.1
Estimates of anaemia prevalence can be affected by the case definition applied and the demographic and health status composition of study samples. Many large, well-characterized community-based studies of older adults, have led to an anaemia prevalence range of 9.2%-23.9% in men, 8.1-24.7% in women (anaemia defined by the World Health Organization as haemoglobin level<12 g/dL in women and <13 g/dL in men)2 Anaemia is in close relationship with a number of chronic medical conditions, most remarkably, chronic kidney disease (CKD), diabetes, and cardiovascular disease (CVD).1 Cardiovascular disease (CVD) is now the most common cause of death worldwide. Before 1900, CVD was responsible for <10% of all deaths. Today CVD accounts for approximately 30% of deaths worldwide, including 40% in high-income countries and 28% in low- and middle-income countries.3 As investigated in the Atherosclerosis Risk in Communities (ARIC) study, anaemia is a potential risk factor for cardiovascular disease outcomes in the general population. In this large, diverse cohort of patients (n=14410) who were not pre-selected for suffering from cardiovascular disease, anaemia predisposed patients to a risk of developing cardiovascular disease and is a risk factor in cardiovascular survival rate.4 Several clinical studies proved that anaemia and low haemoglobin have been associated with diverse outcomes.5 According to a study of 362 hospitalized ambulatory older results, anaemic patients were more likely to fall during hospitalization than non-anaemic ones (56% vs. 38%, P<0.001).6
De Maria found that the combination of heart disease and anaemia present (haemoglobin < 11g/dL) in females was associated with a 3.5 times greater risk of mortality than for nursing home residents without these dual comorbidities.1
Recently, the role of anaemia in heart failure has become a focus of interest as a possible target for therapeutic intervention, while so far the association between anaemia and other cardiovascular diseases has been considered less than previously. Hence, present study was designed to investigate the prevalence of anaemia in some of the cardiovascular diseases including ischaemic heart disease, valvular heart disease, congenital heart disease, heart failure, pulmonary vascular disease, peripheral vascular disease, pericardial, myocardial, and endothelial disease.
Patients and Methods
This multicentre cross sectional study included 12031 adult patients (> 18 years old) who were hospitalized with a diagnosis of cardiovascular disease in East Azarbaijan province (northwest Iran) hospitals between March 2007 and March 2008. The patients\\\' medical records were evaluated retrospectively regarding patients\\\' demographic data, cardiovascular risk factors, clinical and laboratory data, main clinical diagnosis and co-morbidities according to International Disease Control (ICD) version 10.7
In this report the definition of anaemia were used as baseline (on admission in hospital) haemoglobin 13 g/dL for men and 12 g/dL for women based on World Health Organization (WHO) criteria. Clinical diagnosis of hospitalized patients was made by cardiologist or internist (depending on physician availability in hospitals) according to International Disease Control (ICD) version 10. Studied demographic variables were patients\\\' age, gender and body mass index. The patients were also assessed regarding medical history of hypertension, diabetes mellitus, cigarette smoking and history of cardiac and noncardiac surgery. Laboratory tests included haemoglobin and plasma creatinine levels and left ventricular ejection fraction (LVEF). In this study relative frequencies of anaemia in various cardiovascular diseases and different age groups were assessed.
This Research was approvaled by Tabriz medical science ethics committee. Before the sampling, we took a written testimonial from each person who took part in the study.
Collected data was analyzed by using SPSS v. 16.0 for Windows statistical package (SPSS Inc. Chicago; IL). Baseline characteristics were compared between groups of interest using g2 statistics for categorical variables and independent samples t test for continuous variables as appropriate. Results are reported as means ± SD, medians with range or interquartile range, or percentages as appropriate. Multivariable logistic regression method was used to evaluate the relationship of clinical predictors to anaemia, adjusted for significant potential confounders. Final models were achieved via stepwise selection (allowing for entry and staying at the 0.10 significance level) of the candidate variables, a number prespecified: age > 70 years old; history of diabetes; cigarette smoking; history of cardiac and noncardiac surgery; LVEF< 40%; plasma creatinine level> 1.2 mg/dL.
Results
A total of 12031 patients with different cardiovascular disease including ischaemic heart disease, valvular heart disease, congenital heart disease, heart failure, pulmonary vascular disease, peripheral vascular disease, pericardial, myocardial, and endothelial disease were studied. Among this number, 2913 were anaemic and 9118 were non-anaemic. The medical files of patients who were involved in this retrospective study, were reviewed.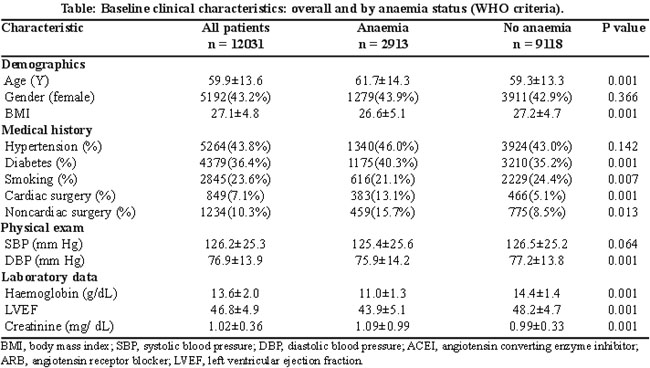
Table-1 lists the characteristics of study patients. There were 5192(43.2%) women (P=0.366), and mean age was 59.9±13.6 years (P=0.001). Patients with anaemia tended to be older (mean 61.7±14.3 vs. 59.3±13.3 years, p=0.001), and have smaller body mass index (26.6±5.1 vs. 27.2±4.7kg/m2, p=0.001); although the differences in body mass index were not significant. Also, anaemic patients were more likely to be hypertensive (46% vs. 43%), diabetic (40.3% vs. 35.2%), and non-smokers (21.1 vs. 24.4). Among 2913 anaemic patients, 388(13.1%) underwent cardiac surgery (p=0.001) compared with 466(5.1%) among 9118 non-anaemic patients (p=0.013).
The mean plasma haemoglobin concentration in the anaemic group was 11±1.3g/dL compared with 14g/dL in non-anaemic group (P=0.001). Overall anaemia was present in 24% of the study population. The average left ventricle ejection fraction (LVEF) in anaemic group was significantly lower than non-anaemic ones (43.9±5.1 vs. 48.2±4.7, p=0.001). Patients with anaemia had higher serum creatinine level compared with non-anaemic individuals (1.01±0.99 vs. 0.99±0.33, P=0.001).
The analysis of prevalence of anaemia among different cardiovascular disease in northwest of Iran led to the data shown in Figure-1.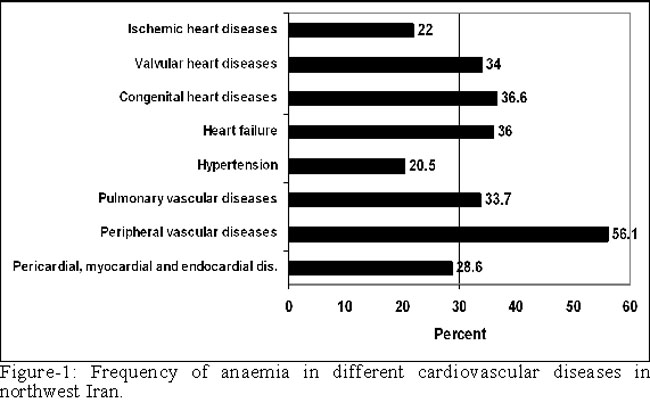
According to our findings, the highest proportion belongs to peripheral vascular disease with the prevalence rate of 56.1%, patients with congenital heart disease are at the second place with the rate of 36.6%, finally heart failure with the rate of 36% takes the third place, while ischaemic heart disease with 22% and hypertension with 20.5% have the lowest prevalence rate. Moreover, this study involves the analysis of anaemia prevalence among different age groups the result of that which is illustrated in Figure-2.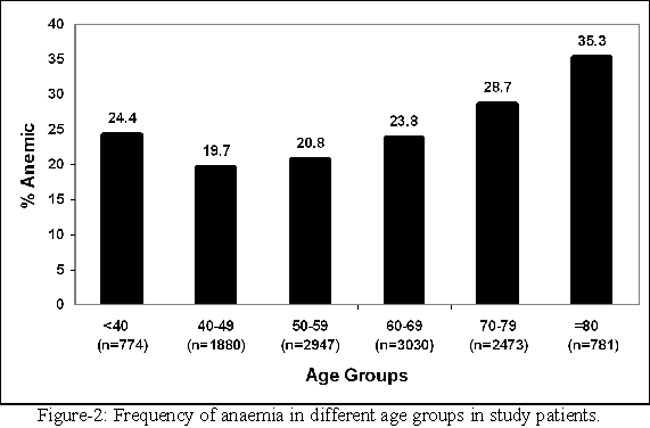
It shows that the prevalence of anaemia increases as a function of age after the 5th decade of life which is a progressive and statistically significant point. In spite of an increase in anaemia prevalence after the age of 50, according to our study it has a considerable prevalence rate before the age of 40 years. Hence, the highest rate of anaemia prevalence in northwest of Iran belongs to the age group older than 70 years and patients younger than 40 years.
Discussion
Over the past decade, it has been proven that anaemia is an emerging risk factor of variety of adverse outcomes in older adults, including hospitalization, disability, and mortality.2 As the explanation of a recent review of epidemiological studies anaemia prevalence rates spread over a wide range, from 3% to 61% among elderly men and from 3% to 41% among elderly women. The variability of rates is dependant on differences in patient populations, criteria used to define anaemia, and study settings.7 In the epidemiologic studies, the most practical definition of anaemia is the one given by the World Health Organization (WHO) (haemoglobin concentration<13 g/dL in men and <12 g/dL in women).2,3 According to the Third National Health and Nutrition Examination Survey (NHANESIII) among community-dwelling adults age 65 years and older WHO-anaemia prevalence was 11.0% in men and 10.2% in women, respectively.2 On the other hand, in a study by Guralnik et al. a rapid rise was found in anaemia prevalence after the age of 50 years, to a rate greater than 20% in persons >85 years.1 This sex differentiation has been reported in other studies as well. In the study on subjects from three US communities (n=3946) who were 70 years of age and older, Salive et al. found that getting older was significantly and independently related with both low haemoglobin level and anaemia. In spite of equal proportion of anaemia in men and women aged 71-74(8.6%), by the use of WHO-definition for anaemia at ages 75-84 years 14.9-15.0% of men and 7.1-12.7% of women were anaemic. In the oldest-age group (85 years and older) the prevalence of anaemia was 29.6-30.7% in men and 16.5-17.7% in women.2 The present study supports previous reports by representing that, there is a progressive significant increase in the prevalence of anaemia with increasing age, particularly after the 5th decade of life. However, our study pointed out high prevalence rate of anaemia among people younger than 40, which is an important point. Over the time, the prevalence of anaemia has increased and this steady rise cannot be easily explained by changes in age and renal function.5 There is growing evidence that anaemia has relationship with cardiac disease and death. Cardiomyopathy pathogenesis related to anaemia has not been ascertained. For example, it is not clear whether the anaemia itself contributes to the development of heart failure. Theoretically, severe anaemia is responsible for inadequate oxygen delivery to tissues, which in the heart could lead to myocyte dysfunction.9,10
In recent years, the prevalence rate of anaemia in patients with chronic heart failure (CHF) has received increasing attention.4 Persistent anaemia usually induces haemodynamic adaptations that finally may lead to left ventricular hypertrophy, exercise intolerance, and cardiac dysfunction. As a result, anaemia may worsen existing heart disease in patients with CHF and affect the outcome of the disease negatively. Furthermore, it has been proven as an independent risk factor for morbidity and mortality in CHF patients.11
Over the past several years, multiple clinical surveys and trials in order to estimate anaemia prevalence rate in CHF patients, have resulted in prevalence ranges from 9.9% in the Valsartan Heart Failure Trial (Val-HeFT) trial to 55.6% in the study by Silverberg.12 This great variation in the results is because of differences in the definition of anaemia and selection of the study populations. In the case of anaemia definition as Hb<11.0 g/dL, 18% of male patients were anaemic. Although with the Hb threshold of 12.0 g/dL, anaemia prevalence in this patient population increased to 33%. (K Swedberg, unpublished data). In a cohort of 1061 patients with advanced CHF (New York Heart Association [NYHA] functional class III or IV; mean left ventricular ejection fraction [LVEF] =22%) was analyzed by Horwich et al. 30% of all patients were anaemic (defined as Hb<13.0 g/dL in men and <12.0 in women g/dL). In one approach, Haemoglobin concentration were divided into quartiles with the range of Hb<12.3 g/dL to Hb<14.8 g/dL. Therefore, depending on the threshold, it led to the prevalence rate of anaemia approximately 25% to 49%. As a remarkable point, the authors found that patients in lower quartiles were tended to be diagnosed with NYHA functional class IV (75.3% of patients in the lowest haemoglobin quartiles). Therefore, anaemia prevalence increases with increasing severity of CHF.13
Considering profile of anaemic patients suffering from CHF in different studies suggests that anaemic patients with CHF are more likely to be older, females, with more severe symptoms and signs of heart failure, greater cardiac functional impairment, higher hospitalization rates, history of diabetes, and renal insufficiency. Hypertension, frequently taking diuretics, and in some studies African-American race and a decreasing blood pressure has been mentioned.4,14 In the current study anaemia was present in 36% of study patients.
Lately, important clinical implications of anaemia in different states of coronary artery disease have been addressed in several studies. It was generally believed that very low levels of haemoglobin could contribute to the occurrence of myocardial ischaemia, in spite of that D.da Silveira and colleagues come to the result that even mild to moderate anaemia stages are linked to increased event rates, symptoms and more medication demand.15 An independent adverse effect of any degree of anaemia on long-term mortality, and post-myocardial infarction was shown by Shu et al. Moreover, in a post-hoc analysis of the TIMI trials by Sabatin et al. an increase in cardiovascular mortality, myocardial infarction, or recurrent ischaemia in NSTEMI patients was not found until haemoglobin concentration dropped below 110 g/L.16 Physiopathologically, there might be a direct relation between anaemia and myocardial ischaemia in CHF patients. Ischaemic heart disease may cause the heart to be more vulnerable to anaemia and in patients with CHF, anaemia may lead to myocardial ischaemia, myocardial stunning, apoptosis, and necrosis. These hypothesis admitted Grigorian Shamagian\\\'s findings that anaemic patients with CHF had higher prevalence rate of heart disease in comparison to non-anaemic ones (54% vs. 35%).17 We found that prevalence of anaemia in ischaemic heart disease was less than other cardiovascular disease. Although, it is beyond the scope of the present study to discuss the various ranges of haemoglobin concentration affect the risk of hospitalization, and mortality, regarding high prevalence risk of hospitalization and mortality in the studies done so far, indicates that treatment of anaemia in ischaemic heart disease may lead to an improvement in relief of symptoms and decrease of mortality risk.
There are scantily available data concerning the prevalence of anaemia in patients suffering from peripheral vascular disease. D.da Silveira et al.15 observed in a prospective cohort of stable coronary artery disease patients that anaemia was a prevalent comorbid condition, associated with unfavorable long-term outcomes. Additionally the authors found that peripheral vascular disease was more common among patients with anaemia compared with non-anaemic ones (18% vs. 9%, p=0.03).13 In the study of anaemia in long-term care (SALT),1 which included 564 nursing home residents, 5% of all patients suffered peripheral vascular disease. Among this 5%, highest percentage belonged to anaemic patients (5% vs. 4%, p=0.622). In our analysis the highest proportion belonged to peripheral vascular disease patients with the prevalence rate of 56.1%.1
There is limited evidence considering the prevalence of anaemia in patients with valvular heart disease. The only available data concerning the subject has been reported by Fyeza Hasan18 in a case-report study of Aortic stenosis and gastrointestinal bleeding. Iron deficiency anaemia and calcefic aortic stenosis in elderly patients are two common findings. Heyde\\\'s syndrome known as the association of aortic stenosis and gastrointestinal bleeding is the rare condition causing iron deficiency anaemia. A possible reason for the bleeding in Heyde\\\'s syndrome is due to aquired form of von Willebrand\\\'s disease (typeIIa) which is result of the aortic stenosis. A recent study showed that 21% of patients suffered severe aortic stenosis experienced skin or mucosal bleeding. Most of the patients had vWF abnormalities, the severity of which ascertained by the degree of stenosis.18 In our study, anaemia is nearly common with the prevalence rate of 34% in patients with valvular heart disease considering anaemia prevalence after peripheral vascular disease, congenital heart disease, and heart failure.
A useful validated screening method for pulmonary hypertension is the measuring of tricuspid valve regurgitant jet velocity by echocardiography of pulmonary artery pressure in adult patients with sickle cell disease.19
Using echocardigraphy and describing pulmonary hypertension as a tricuspid regurgitant jet velocity > 2.5 m/s, the prevalence of pulmonary hypertension in patients with Sickle Cell Disease (SCD) approaches 30%.20 In a recent autopsy studies, up to 75% of patients suffered SCD, at the time of death, have histologic evidence of pulmonary arterial hypertension.21
Conclusion
In overalls 24% of our cardiovascular disease patients had anaemia. Anaemia was more prevalent before 40 and after 70 years age. We found that anaemia was more common among patients with peripheral vascular disease, then CHD and CHF. History of surgery, non-smoking, lower LVEF and higher serum creatinine level increase the incidence of anaemia.
Acknowledgements
The authors gratefully acknowledge the excellent assistance of all medical personnel who helped us to successfully complete this study.
References
1.Pandya N, Bookhart B, Mody SH, Funk Orsini PA, Reardon G. Study of anaemia in long-term care (SALT): prevalence of anaemia and its relationship with the risk of falls in nursing home residents. Curr Med Res Opin 2008; 24: 2139-49.
2.Patel KV. Epidemiology of anaemia in older adults. Semin Hematol 2008; 45: 210-7.
3.Fauci A, Braunwald E, Kasper D, Hauser S, Longo D, Jameson J, et al. Harrison principle\\\'s of internal medicine.17th ed. New York: McGraw publishing Co, 2008.
4.Komajda M. Prevalence of anaemia in patients with chronic heart failure and their clinical characteristics. J Card Fail 2004; 10: S1-4.
5.Dunlay SM, Weston SA, Redfield MM, Killian JM, Roger VL. Anaemia and heart failure: a community study. Am J Med 2008; 121: 726-32.
6.Dharmarajan TS, Avula S, Norkus EP. Anaemia increases risk for falls in hospitalized older adults: an evaluation of falls in 362 hospitalized, ambulatory, long-term care, and community patients. J Am Med Dir Assoc 2006; 7: 287-93.
7.International Statistical Classification of Diseases, 10th revision, clinical modification (ICD-10). (Online) 2011 (Cited 2011 May 15). Available from URL: http://www.cdc.gov/nchs/icd/icd10cm.htm.
8.Ble A, Fink JC, Woodman RC, Klausner MA, Windham BG, Guralnik TM, et al. Renal function, erythropoietin and anaemia of older persons: the In Chianti Study. Arch Intern Med 2005; 165: 2222-7.
9.Riva E, Tettamanti M, Mosconi P, Apolone G, Gandini F, Nobili A, et al. Association of mild anaemia with hospitalization and mortality in the elderly: the Health and Anaemia population-based study. Haematologica 2009; 94: 22-8.
10.Heode N, Rich MW, Gayomali C. The cardiomyopathy of iron deficiency. Tex Heart Inst J 2006; 33: 340-4.
11.Anand IS, Chandrashekhar Y, Ferrari R, Poole -Wilson PA, Harris PC. Pathogenesis of edema in chronic severe anaemia: studies of body water and sodium, renal function, haemodynamic variables and plasma hormones. Br Heart J 1993; 70: 357-62.
12.Silverberg DS, Wexler D, Iaina A. The importance of anemia and its orrection in the management of severe congestive heart failure. Eur J Heart Fail 2002; 4: 681-6.
13.Horwich TB, Fonarow GC, Hamilton MA, McLellan WR, Borenstein J. Anaemia is associated with worse symptoms, greater impairment in functional capacity and significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol 2002; 39: 1780-6.
14.Adams KF, Patterson JH, Oren RM, Mehra MR, O\\\'Connor CM, Pina IL, et al. Prospective assessment of the occurrence of anaemia in patients with heart failure: results from the Study of Anaemia in a Heart Failure Population (STAMINA-HFP) Registry. Am Heart J 2009; 157: 926-32.
15.daSilveira AD, Ribeiro RA, Rossini AP, Stella SF, Ritta HA, Stein R, et al. Association of anaemia with clinical outcomes in stable coronary artery disease. Coron Artery Dis 2008; 19: 21-6.
16.Shu DH, Ransom TP, O\\\'Connell CM, Cox JL, Kaiser SM, Gee SA, et al. Anaemia is an independent risk for mortality after acute myocardial infarction in patients with and without diabetes. Cardiovascular Diabetology 2006; 5: 8.
17.Grigorian Shamagian L, Varela Roman A, Garcia-Acuna JM, Mazon Romos P, Virgos Lamela A and Gonzalez-Juanatey JR. Anaemia is associated with higher mortality among patients with heart failure preserved systolic function. Heart 2006; 92: 780-4.
18.Hasan F, O\\\'Brien CS, Sanyal A, Dalton HR. Aortic stenosis and gastrointestinal bleeding. J R Soc Med 2004; 94: 81-2.
19.Anthi A, Machado RF, Jison ML, Da AT, Taveira-dasilva AM, Rubin LJ, Hunter et al. Hemodynamic and Functional Assessment of Patients with Sickle Cell Disease and Pulmonary Hypertention. Am J Respir Crit Med 2007; 175: 1272-9.
20.Gladwin MA, Sachdev V, Jison ML, Shizukuda Y, Plehn JF, Minter K, et al. Pulmonary hypertention as a risk factor for death in patients with sickle cell disease. N Engl J Med 2004; 350: 886-95.
21.Haque AK, Gokhale S, Rampy BA, Adegboyega P, Duate A, Saldana MJ. Pulmonary hypertention in sickle cell hemoglobinopathy: a clinicopathologic study of 20 cases. Hum Pathol 2002; 33: 1037-43.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: