
Lin Xu ( Department of Orthopaedics, Changzheng Hospital, Second Military Medical University, Shanghai, China. )
Fei Huang ( Department of Human Anatomy, Binzhou Medical University, Yantai, China. )
Chunlin Hou ( Department of Orthopaedics, Changzheng Hospital, Second Military Medical University, Shanghai, China. )
November 2011, Volume 61, Issue 11
Original Article
Treatment for Carpal Tunnel Syndrome by Coronal Z-type Lengthening of the Transverse Carpal Ligament
Abstract
Objective: To compare the effects of coronal Z-type lengthening of transverse carpal ligament with conventional open approach for carpal tunnel syndrome.
Methods: A double-blinded study was conducted from January 2005 to August 2008 on 68 patients with a mean age of 41 years (range 27~55 years) diagnosed as severe carpal tunnel syndrome. They were randomized into two groups(A and B). Patients in group A underwent coronal Z-type lengthening of transverse carpal ligament, and patients in group B had conventional open approach surgery. Postoperative evaluation was scheduled at 1, 3, 6 and 12 months after the surgery and incidence rate of bowstring of the flexor tendons, improvement of grip strength and ADL activities of daily living) score were recorded.
Results: Fifty-eight patients had been followed up successfully, 30 and 28 for group A and B respectively. The Scar Tissue Formation of the flexor tendons in group B was observed more than that in group A at 6 and 12 month after operation. Improvement of grip strength were observed in two groups, which was statistically different between 6 and 12 months after operation and no significant difference was seen between 1 and 3 months after operation. According to ADL, the satisfaction rates documented on form for patients were statistically different in the two groups at 6 and 12 months after operation and no difference was noted at 1 and 3 months after operation.
Conclusion: Excellent improvement of function and satisfaction were achieved by Coronal Z-type reconstruction of the flexor retinaculum for severe carpal tunnel syndrome. Our method offers a more effective alternative method for conventional carpal tunnel open decompression surgery.
Keywords: Carpal tunnel syndrome, Median nerve, Reconstruction (JPMA 61: 1068; 2011).
Introduction
Carpal tunnel syndrome (CTS) is a disorder caused by compression at the wrist of the median nerve supplying the hand, causing numbness and tingling. CTS is a common peripheral nerves entrapped disease with only treatment of transverse carpal ligament cutoff. Although surgery under arthroscopy or minimally invasive surgical technology has many advantages such as minimal wound, faster recovery, the 1/3 severe CTS left still need conventional open decompression surgery to treat. Transverse carpal ligament was damaged unavoidably in conventional open decompression surgery, leading to unstable bony structure of carpal canal, bowstring of flexor tendon, permanent attenuated grip strength, even loss of work capacity for young workers.1 Accordingly, based on researches of anatomy and images, we developed the coronal Z-type lengthening of transverse carpal ligament for young patients with severe CTS and got better clinical effect.
Patients and Methods
Sixty-eight patients with severe CTS confirmed by clinical physical examination and electromyogram were enrolled, male 42, female 26, and 54 and 14 cases with right and left hand affected respectively. These patients were randomly assigned into group A and B, 34 cases respectively. Group A had 19 males and 15 females; whereas group B had 23 males and 11 females. Patients in group A received the surgery of coronal Z-type lengthening of transverse carpal ligament, and patients in group B underwent conventional open decompression approach. The study was double-blinded. Postoperative evaluations were scheduled at 1, 3, 6 and 12 months after operation, and incidence rate of malformation of flexor tendon, improvement of grip strength, ADL (activities of daily living) were recorded.
To keep the operation field clear, the pneumatic tourniquet was fixed on the upper arm of affected limb. Anaesthesia of brachial plexus block was employed. In group A, Z-type lengthening of transverse carpal ligament was conducted. Sigmoid incision with 6cm length on palmar surface of wrist, after skin and subcutaneous tissue was cut-off, free skin flap about 2.5cm bilaterally, avoiding injury to the superficial palmar branch of median nerve was formed. After the transverse carpal ligament was exposed, a longitudinal section 1.5mm deep at the ulnaris of the ligament was done. The distance between the incision and middle point of the ligament was 1 cm. The incision in the vertical direction paralleled with the ligament, and went through the middle point of the ligament and ended at the radialis of the ligament. The distance between ending point and middle point was also 1cm, and then the ligament was cut-off at the ending point longitudinally. Care was taken not to injure the recurrent branch of median nerve. The median nerve was carefully explored, and compression factors were relieved. If needed, epineurium or lamellar sheath was released, then the transverse carpal ligament was stretched transversally and the extended ligament was sutured. A 0.5cm tissue overlapped, then 5-0 atraumatic suture was used to fix the transverse carpal ligament and 3-0 suture lines was used to fix the skin. In this surgery, the transverse carpal ligament can be extended as long as about 1cm. In group B, firstly the transverse carpal ligament was exposed, then it was cut-off in the middle point longitudinally. Later the ligament would retract because of the tension, and a gap about 0.5-1cm width would be formed. After the median nerve was decompressed, the skin was sutured with 3-0 suture lines directly (Figure).
After bandage, the wrists in both groups was fixed with dorsal wrist plaster slab in neutral position.
The improvement of grip strength, incidence rate of bowstring of the flexor tendons and ADL score were evaluated with SPSS software.
Results
Thirty patients in group A and 28 patients in group B were followed. Scar Tissue formation of the flexor tendons was not seen at 1 and 3 month after the operation in both groups. This deformation was encountered in 1 case in group A , 11 in group B at 6th month after operation, and 8 patients in group A, 26 cases in group B at 12th month after operation (Table-1).
The grip strength of affected hands before operation in group A and B was 7±1.1kg and 4.5±1.5kg separately, and the corresponding grip strength of healthy hands was 49±7.5kg and 47±7.0kg separately. At 1st, 3rd, 6th, 12th month after operation, the grip strength improved apparently, which was 8.5±1.2 kg, 20.8±1.4 kg, 39.6±7.5 kg, 38.4±6.4 kg in group A and 7.9±1.0 kg, 19.2±1.2 kg, 21.4±6.2 kg, 22.6±4.5 kg in group B, but there was no significant difference for recovery rate of grip strength between 1st month and 3rd month (recovery rate of grip strength=grip strength of affected hand after operation - grip strength of affected hand before operation/the grip strength of corresponding healthy hand); and the recovery rate of grip strength was different significantly at 6th and 12th month after operation (Table-2).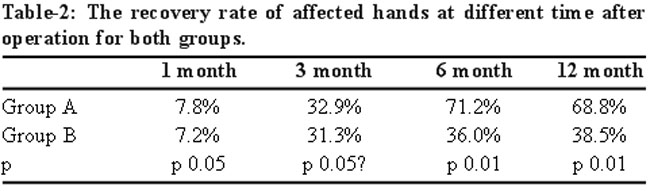
The satisfaction rate was statistically different in the two groups at 6th and 12th months after operation and no difference at 1st and 3rd month (Table-3).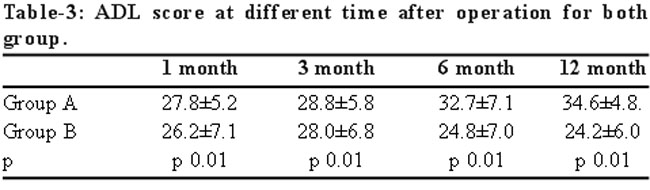
Discussion
Carpal tunnel syndrome(CTS) was described by James Paget2 firstly in 1865. In 1933, the release of transverse carpal ligament was used to treat CTS for the first time by Jamse learmonth.3 For nearly one century, cut-off of transverse carpal ligament was the only method to treat CTS, which was refractory to expectant treatment. There were three modus operandi for surgery of release of carpal tunnel for nerve decompression: conventional open decompression, open decompression under arthroscopy of wrist, and minimally invasive open decompression. An open decompression under arthroscopy of wrist or minimally invasive open decompression were good for mild to moderate CTS, however for severe CTS, the methods mentioned above were not satisfactory.4,5 Conventional open decompression surgery can fully expose carpal tunnel and median nerve, which was the only option for severe CTS. However, conventional surgery cannot repair transverse carpal ligament, and sometimes part of transverse carpal ligament was removed, leading to Scar Tissue Formation of the flexor tendon. Wrist flexion and permanent weakness of grip strength can influence living and work abilities for young people severely, so many labourers lost their work.
Transverse carpal ligament is an important structure for wrist to maintain the mechanical effect of flexor tendons and can protect muscle tendons and nerves in carpal canal. Change in the direction of movement of tendons plays an important role in biomechanical effect of tendons.6 Forward7 reported that when transverse carpal ligament was totally severed, the Scar Tissue Formation of flexor tendons formed apparently. Therefore, it is the consensus of researchers that reconstruction of transverse carpal ligament after total cut-off was essential.8 Mathoulin9 reestablished the transverse carpal ligament with skin flap transplantation in corpses, which can increase the volume of carpal tunnel by about 40.92% and prevent bowstringing of flexor tendon effectively. Lee Berger10 conducted inflatable extension of transverse carpal ligament with 75% satisfaction rate, and most patients went back to work in two weeks. However, some researchers got the opposite conclusion that there was no significant difference between reconstruction of transverse carpal ligament, especially for older patients, with extension in sagittal plane.11 In this study, the extension surgery in coronal plane not only augmented carpal tunnel volume, but reconstructed the anatomic structure of transverse carpal ligament and carpal tunnel. We also found that when transverse carpal ligament was totally cut-off in conventional surgery, the incidence rate of bowstringing of the flexor tendons was 92.9%, and grip strength of affected hand was significantly weaker than the healthy hand. Besides, 1 month and 3 months after surgery, bowstringing of the flexor tendons did not happen in cut-off group or reconstruction group, which may be due to the scarification, but at 6 months and 12 months after surgery, the cases with bowstringing of the flexor tendons in reconstruction group was 1 and 8 respectively. The reason may be over extension of transverse carpal ligament, too early and too widely use of affected hand, and laceration of reconstructed transverse carpal ligament. Therefore, the optimum extension length for transverse carpal ligament was about 1cm, and the time for weight loading of the affected hand was more than 3 months.
The grip strength of affected hand recovered slowly after 1 month and 3 months of the surgery, which may be caused by the soreness and fixation of tendons, but 6 months and 12 months after the operation, the grip strength improved, and reconstruction was better. There is no significant difference for ADL score between the two groups after 1 and 3 months, dissatisfaction for grip strength and soreness within 1 month after surgery may be the main reasons. ADL score was different significantly between the two groups after 6 and 12 months respectively, and the satisfaction rate was better in reconstruction group in which complications of surgery related scaring, bowstringing of flexor tendon, responsive sympathetic dystrophy and rigidity of wrist joint was less. Besides, morbidity of pillar pain was lower in reconstruction group because of less cutaneous nerve depression. No vessels and nerves were injured and no serious infection occurred in both groups. However, one case in reconstruction group relapsed, and symptoms disappeared after the second surgery, which may be caused by insufficient extension of the transverse carpal ligament.
Conclusion
In conclusion, compared with conventional open decompression surgery, the characters of coronal Z-type lengthening of the transverse carpal ligament included; restoring normal anatomy of carpal tunnel, stable construction of carpal tunnel, keeping trochlear function of transverse carpal ligament to flexor tendon, preventing bowstringnig of flexor tendon and restoring grip strength.
Acknowledgement
This research was supported by programme for New Century Excellent Talents in University, NCET. (No.NCET-08-0876) and a project from Shandong Natural Science Foundation (Y2008C18).
References
1.No author listed. Management of carpal tunnel syndrome. Drug Ther Bull 2009; 47: 86-9.
2.Gross C LJ, Nelson A. Carpal tunnel syndrome:a review of the literature with recommendations for further research. Florida J Public Health 1998; 9: 22-8.
3.Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosen I. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999; 282: 153-8.
4.Mondelli M, Giannini F, Giacchi M. Carpal tunnel syndrome incidence in a general population. Neurology 2002; 58: 289-94.
5.Buchberger W, Schon G, Strasser K, Jungwirth W. High-resolution ultrasonography of the carpal tunnel. J Ultrasound Med 1991; 10: 531-7.
6.Stevens JC, Smith BE, Weaver AL, Bosch EP, Deen HG Jr, Wilkens JA. Symptoms of 100 patients with electromyographically verified carpal tunnel syndrome. Muscle Nerve 1999; 22: 1448-56.
7.Forward DP, Singh AK, Lawrence TM, Sithole JS, Davis TR, Oni JA. Preservation of the ulnar bursa within the carpal tunnel: does it improve the outcome of carpal tunnel surgery? A randomized, controlled trial. J Bone Joint Surg Am 2006; 88: 2432-8.
8.Mashoof AA, Levy HJ, Soifer TB, Miller-Soifer F, Bryk E, Vigorita V. Neural anatomy of the transverse carpal ligament. Clin Orthop Relat Res 2001; 386: 218-21.
9.Mathoulin C, Bahm J, Roukoz S. Pedicled hypothenar fat flap for median nerve coverage in recalcitrant carpal tunnel syndrome. Hand Surg 2000; 5: 33-40.
10.Garcia-Elias M, Sanchez-Freijo JM, Salo JM, Lluch AL. Dynamic changes of the transverse carpal arch during flexion-extension of the wrist: effects of sectioning the transverse carpal ligament. J Hand Surg Am 1992; 17: 1017-9.
11.Sucher BM, Hinrichs RN. Manipulative treatment of carpal tunnel syndrome: biomechanical and osteopathic intervention to increase the length of the transverse carpal ligament. J Am Osteopath Assoc 1998; 98: 679-86.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: