
Nilufer Cetisli Korkmaz ( Pamukkale University, School of Physical Therapy and Rehabilitation, Denizli, Turkey. )
Nuray Kirdi ( Hacettepe University, Faculty of Health Sciences, Department of Physical Therapy and Rehabilitation, Ankara, Turkey. )
Cagri Mesut Temucin ( Hacettepe University, Institute of Neurological Sciences and Psychiatry, Ankara, Turkey. )
Kadriye Armutlu ( Hacettepe University, Faculty of Health Sciences, Department of Physical Therapy and Rehabilitation, Ankara, Turkey. )
Yavuz Yakut ( Hacettepe University, Faculty of Health Sciences, Department of Physical Therapy and Rehabilitation, Ankara, Turkey. )
Rana Karabudak ( Hacettepe University, Faculty of Medicine, Department of Neurology, Ankara, Turkey. )
August 2011, Volume 61, Issue 8
Original Article
Abstract
Objective: To examine the effects of High Voltage Pulsed Galvanic Stimulation (HVPGS), that was applied to the spasticity associated weakness in knee flexors and ankle dorsiflexors, on strength and fatigue, in Multiple Sclerosis (MS) patients, in a non-randomized controlled trial.
Methods: A total of 33 MS patients were included. Fatigue and strength were analyzed with 3rd and 30th second data by dynamometric measurements synchronously with surface electromyography (EMG) [power spectrum analysis (amplitude, mean frequency, median frequency and root means square]. In the experimental group HVPGS and in the control group repetitive contractions from Proprioceptive Neuromuscular Facilitation (PNF) technique were applied for 18 treatment sessions.
Results: In both groups and all muscle groups, dynamometric measurement and EMG results in the 30th second were significantly lower according to in the 3rd second before and after the treatments. Both strength and fatigue improved after the treatment both in the HVPGS and PNF group.
Conclusion: It was concluded that, MS patients have both central and peripheral fatigue. FO2 localized and intensive effects in strength and fatigue, HVPGS was more impressive than the PNF. PNF was more effective to obtain general effects. Moreover, the application of HVPGS with other rehabilitation techniques may be more appropriate and effective.
Keywords: Multiple Sclerosis (MS), Strength, High Voltage Pulsed Galvanic Stimulation (HVPGS), Proprioceptive Neuromuscular Facilitation (PNF) (JPMA 61:736; 2011).
Introduction
Multiple sclerosis (MS) is a demyelinating disease of the central nervous system and at the same time it causes axonal injury that can result in impaired motor function, increased symptomatic fatigue, skeletal muscle weakness, and excessive skeletal muscle fatigue. The phenomenon of fatigue can be studied as peripheral (motor), central and subjective fatigue.2 While fatigue can be defined in association with pathophysiology and symptoms of MS, it is also, unfortunately, one of the most difficult symptom and complex phenomenon to treat and to understand.2,3
Fatigue is a ubiquitous phenomenon, abnormal only when it occurs under circumstances that should not produce it. The psychological disinclination to exert one is common after a late night of over-indulgence. Equally, when performing strenuous tasks, there will be increasing inability to generate the force required to perform the task due to a failure of force production at muscle level (\\\'\\\'peripheral fatigue") or a failure to sustain the required neural drive to muscle ("central fatigue"). It is likely that both extremes of the fatigue spectrum are important in multiple sclerosis. On the one hand, disease load could impose physical and cognitive constraints that lead to a mismatch between the perception of the force that is exerted and the actual force required to maintain or repeat the task. On the other hand, the \\\'\\\'motor" phenomenon, in which there is the increasing inability to generate, sustain or repeat a contraction, will accentuate any weakness (and may be a feature of the temperature-induced aggravation of deficit in Uhthoff\\\'s phenomenon or exercise-induced weakness).4
For many years, patients with multiple sclerosis (MS) have been advised to avoid exercise because of excessive fatigue and thermosensitivity.3 Comprehensive physiotherapy and rehabilitation programmes utilizing exercises to decrease the spasticity and perceived fatigue, maintain or improve range of motion, antagonist muscle strength, endurance, and balance, improve the MS patients\\\' functional status. Neuromuscular electrical stimulation (NMES) and proprioceptive neuromuscular facilitation (PNF) were the most important applications for these aims.3,5
Electrical currents have been used to restore motor function. A major aim of stimulation is that it preserves and provides the activation of inhibited muscle groups. As a result of increased activity (i.e., chronic electrical stimulation or training), properties of fast muscles and fibers shift to those with slower and more oxidative characteristics. By therapeutic electrical stimulation with High Voltage Pulsed Galvanic Stimulation (HVPGS), recovery was better and faster in increasing the tolerance to the muscle fatigue and preventing the atrophy in muscle fibers (Type II).6,7
Proprioceptive neuromuscular facilitation (PNF) technique was firstly developed for and applied to the MS patients for many years. PNF aims to facilitate the voluntary effort by the basis of facilitating the activity of neuromuscular mechanism with stimulating the proprioceptors. If the PNF techniques have the cumulative effect of facilitation, then it has value in neuromuscular re-education.8
The purpose of this prospective study was to determine the type of fatigue, if it is peripheral or central fatigue or both, in MS patients. Additionally, the fact that none of the previous studies in MS have attempted to show the effects of HVPGS, the purpose of this non-randomized controlled trial was to examine the effects of HVPGS, which was applied to the spasticity associated weakness in knee flexors and ankle dorsiflexors, on fatigue and strength in MS patients.
Subjects and Methods
In presence of some inclusion criteria [diagnosis of clinically definite MS, score of 1.0-6.5 on the Expanded Disability Status Scale (EDSS), no relapse for at least 3 months before baseline, and were not using immunosuppressive, fatigue and muscle relaxant treatment or no dose changes were made during the study] 33 volunteer MS patients were recruited with non-randomized method and participated in this investigation after giving their written consent. Research was approved by the Medical, Surgical and Medicine Researches Ethics Committee of Hacettepe University (approval no: LUT 05/19-9 in 17.02.2005).
In the experimental group, HVPGS was applied to strengthen weak knee flexor and ankle dorsiflexor muscles, while in the control group PNF was applied. The mean age of 16 (12 women, 4 men) subjects\\\' was 41.81±8.43 years in the HVPGS group; in the control group 17 (7 women, 10 men) subjects\\\' mean age was 36.24±10.08 years (Table-1).
Subjects underwent the set of clinical tests. All tests were done before and after the 18 treatment sessions. Their disability levels were determined by using EDSS. Ambulation levels were investigated with Hauser Ambulation Index (AI).9
Dynamometric Measurements and Power Spectrum Analysis with Surface Electromyography
In assessing the peripheral, central and subjective fatigue, many different techniques could be used.2,5,10,11 The simplest method is to compare the maximal strength at the beginning and end of contraction.10,12 Although subjects trained isotonically, isometric testing was performed because it is reliable. During maximal voluntary contraction, as the amount of force declines, the changes can be seen objectively by the spectral EMG analysis.2 The classical methods used to extract information rely on surface EMG temporal analysis [root mean square (rms), of the signal to describe the energy] and on EMG frequency parameters [mean frequency (mnf), median frequency (mdf)].13,15
To determine the type of fatigue that could be seen in MS patients and if there were any differences for fatigue and strength in muscle quadriceps femoris (QF) and muscle tibialis anterior (TA) between pre and post-treatments in the groups and any differences between the HVPGS and PNF treatment groups; subjects\\\' fatigue was analyzed with amplitude (amp), mnf, mdf and rms values in surface EMG by power spectrum analysis. Also, 3rd and 30th sec\\\'s data were analyzed in dynamometric isometric measurements synchronously with surface EMG data.
The order of testing procedure remained consistent throughout the study. For isometric contraction resistance was given from 1/3 proximal of tibia for QF and dorsomedial of foot for TA. If any record could not be taken or the patient did any compensation during contraction the test was stopped.
Subjects were divided into two groups. HVPGS was applied in the study group and PNF was applied to the control group for totally 18 treatment sessions (3 days a week for 6 weeks).
HVPGS was applied by using "GV 350-Galvanic Stimulator". The stimulator gives 100µsec pulse width automatically; pulse frequency was settled as 60pulse/sec. Not to cause fatigue interrupted form was chosen in which there were 5sec impulse and 5sec rest periods. The amplitude was increased till a contraction can be seen without any discomfort to the patient. With 3min rest period totally 20min HVPGS was applied.
In the literature it was stated that the most common techniques and PNF appear to be of roughly equal efficacy in MS patients, despite their different rationale. In patients with arm paresis or trunk instability, proprioceptive facilitation techniques may be used for the amelioration of muscle tone and in neurophysiological concept and behavioural techniques for postural adjustment, breathing strategies, feedback methods and fatigue. Additionally, therapeutic exercises with \\\'proprioceptive re-education\\\' are recommended for reduction of pain in MS patients.16 For these reasons we prefer to treat control group MS patients with PNF. Repeated contractions technique from PNF was applied with 10 repetitions. We applied as range of motion instead of pattern, not to cause any compensation or fatigue in MS patients.
For all statistical analyses, differences were considered significant at p<0.05. The demographic characteristics, EDSS and AI scores, 3rd and 30th sec\\\'s data of power spectrum analysis and dynamometric measurement were analyzed with the non-parametric Mann-Whitney U test to determine the differences between the groups. To record the improvements all data were analyzed with non-parametric Wilcoxon-Rank test.
Results
There were no differences between the groups at baseline in either subject characteristics or EDSS or AI scores (p>0.05) (Table-1).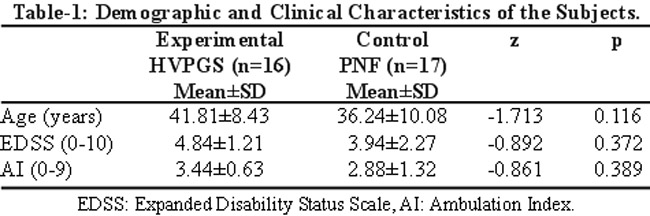
For the pre-treatment results, the significant difference between the groups were seen only in 3rd and 30th sec mnf and mdf value (p<0.05), while there was not any difference for the other values for right and left QF (p>0.05) (Table-2).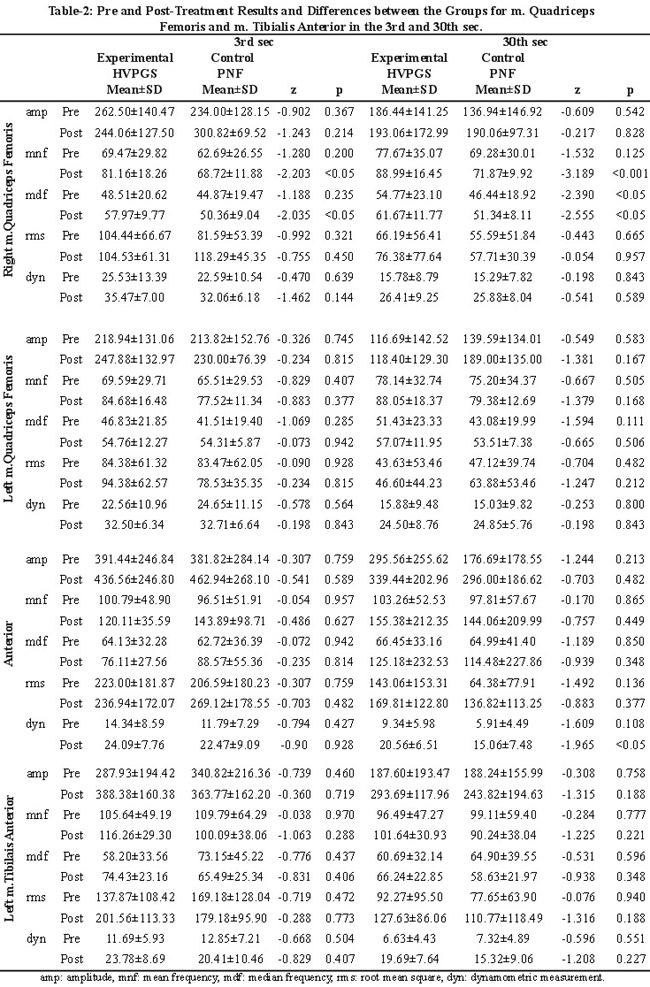
We obtained significant differences only for the 3rd sec rms in the right QF (p<0.05) and 3rd sec mdf in the left QF (p<0.01) of PNF group. However, the post-treatment results were higher than the pre-treatment results, no difference were noted in the rest of the data (p>0.05) (Table-3).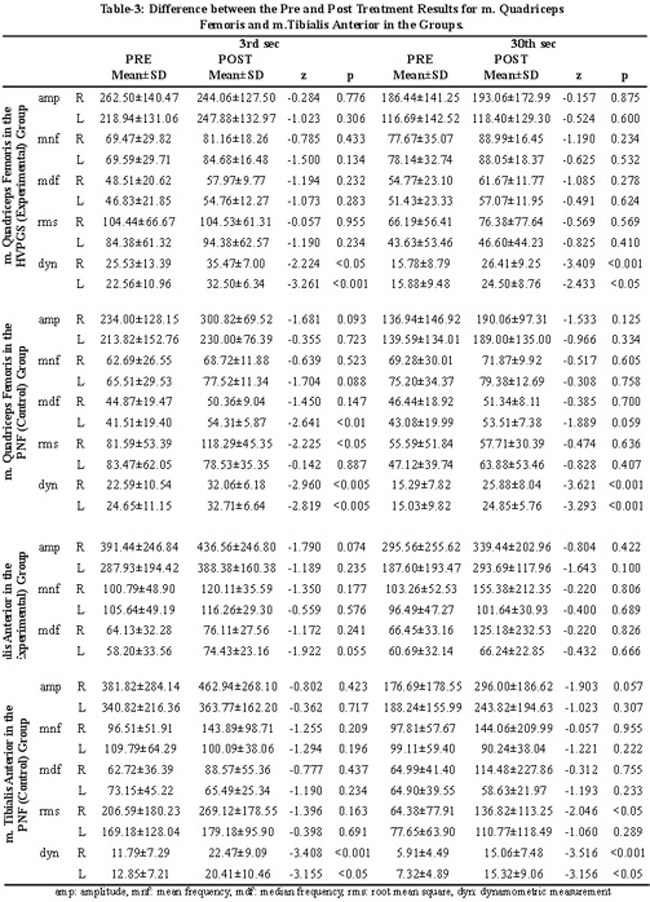
All dynamometric measurement data were significantly increased in the post-treatment results for both sides of QF. For the right side it increased in the 30th sec from 15.78 8.79kg to 26.41 9.25kg (p<0.001) in the HVPGS group (Table-3). Meanwhile left side QF results were significantly increased both in HVPGS and PNF groups, too (p<0.05). But difference could not be obtained between the groups (p>0.05) (Table-2).
Any differences were recorded between the groups for the TA (p>0.05) (Table-2). Interestingly, significant difference was determined between pre and post-treatment results in the PNF group just for the 30th sec rms of the right TA (p<0.05), while no differences were recorded for the rest of them (p>0.05) (Table-3). All dynamometric measurement values were increased significantly after the treatment for both sides of QF and TA (p<0.05) (Table-3).
Discussion
The management of fatigue must initially focus on identifying whether or not the symptom of fatigue is accompanied by the development of weakness, and then treating all factors that can contribute to that feeling. Although, several controlled studies have reported a reduction in fatigue with rehabilitation programmes, the evidence for effectiveness of aerobic exercise in treatment of fatigue is inconsistent, and larger trials with more rigid experimental designs are required to address this issue.4 Assessing the effectiveness of rehabilitation is particularly difficult in MS patients. First of all, the activity and the course of the disease are difficult to measure reliably. Furthermore, the symptom patterns can fluctuate.17 All these make MS, one of the most difficult chronic conditions to conduct meaningful specific guidelines for type, duration and intensity of physiotherapy and rehabilitation programmes.
Many studies in MS literature attest to the value of an integrated, comprehensive, and intensive rehabilitation programme for patients with MS.2,3,17-20 Kesselring and Beer reported that despite newer immunomodulating therapies, symptomatic treatment and rehabilitation are effective, even though the rehabilitation has no direct influence on underlying disease activity or progression.17 Interestingly, there was no study about the effects of HVPGS on strength and fatigue in MS patients. In general, there were spasticity in extensor group muscles and weakness in flexor group muscles of lower extremity in MS patients, which have huge negative influences during walking. Due to these, we planned a rehabilitation programme which included HVPGS or PNF application to strengthen without causing any fatigue symptom.
Sharrack and colleagues stated that the EDSS is the best known and the most widely used scale, but its sensitivity to clinical changes is weak.21 To determine the disability and mobility levels we used AI in addition to EDSS. It was seen that, EDSS and AI were not able to differentiate between individuals at one point in post-treatment time and detect changes in disability. In the future studies, more sensitive scales could be used for disability level.
Accepting restrictions in coverage, it is important to distinguish \\\'\\\'peripheral" fatigue from \\\'\\\'central" fatigue. The former refers to fatigue of the force-generating mechanism within muscle (peripheral fatigue), while the latter refers to a decline in the neural drive to muscle and, theoretically at least, this could have supraspinal and spinal contributions and even be due to conduction block in motor axons in the peripheral nerve (central fatigue).4
Comparing the maximal strength at the beginning and the end of contraction with 30sec duration is the simplest conventional approach in the literature.10-12 Svensson, Gerdle and Elert determined that in several endurance studies, dynamometry has been combined with EMG recordings.22 In our non-randomized controlled trial, to determine the fatigue, 3rd and 30th sec\\\'s data of amp, mnf, mdf and rms by power spectrum analysis were used. We also analyzed dynamometric isometric measurements synchronous with these.
Changes in mnf and mdf are common methods for expressing peripheral fatigue by frequency shift during sustained contractions. There is strong evidence that the surface EMG power spectrum shifts towards lower frequencies mainly as a result of the decrease in MU conduction velocity associated with fatigue.14,23 In our groups and all muscle groups, amp and rms of spectrum analysis in the 30th sec were significantly lower according to in the 3rd sec before and after the treatments. These pre-treatment results showed that all subjects were fatigued during 30 sec isometric contraction. We accept them as a proof for peripheral fatigue and our first main result.
Svensson, Gerdle and Elert said that by combining dynamometry and mnf, the origin of the decrease in mechanical performance (central or peripheral) can be determined. Hence, a decrease in mechanical output without a shift in mnf toward lower frequencies is most likely to be of central origin.22 In our non-randomized controlled trial there was not any decrease in mnf or mdf values except for left TA. Meanwhile, there were significant decreases during the test time in all values for dynamometric measurements in both groups\\\' before and after treatment results. There was a decrease in motor performance without a shift through the lower frequencies. It was concluded that, in MS patients, who were included in our study, have got fatigue with central origin, too. These findings are consistent with fatigue of mainly central origin, which is the second most important result of our study. MS patients also have difficulties in recruiting their type II MUs (associated with decreased strength) and relied primarily on the type I fibers.22
To investigate whether neurorehabilitation is able to influence clinical parameters and brain function in seventeen patients with MS Rasova et al worked on known principles of sensorimotor learning and adaptation. They employed various elements of several treatment methods in an eclectic way and one of them was PNF. They stated that patients who underwent neurorehabilitation showed a greater drop in fatigue, depression, impairment, disability and handicap and more improvement in quality of life than those who did not receive therapy.24 In another study the patients who participated in one of training programme showed a significant improvement in comparison to those who did not change their present habits. Especially, the neurophysiologically based physiotherapy with PNF had the greatest impact on impairment, and the aerobic training on spirometric and spiroergometric parameters. They also stated that all methods (the neurophysiologically based physiotherapy with PNF, the aerobic training and the combined programme) had an impact on fatigue.25 Our results were also marking the same results with the literature in MS patients. We found that the strength of both quadriceps femoris and tibialis anterior muscles measured with dynamometer in 3rd and 30th sec were increased significantly in control group MS patients who were treated with PNF.
When Rousseaux and Dominie reviewed the literature, they determined that neuromuscular facilitation can be used with substantial benefit on mobility and balance, as well as on gait, when patients are still able to walk.26 In spite of the differences between normal and electrically induced activity, imposed electrical activity has certain advantages compared to exercise or other protocols increasing muscle activity. First, the rigid hierarchical order of MU recruitment is bypassed and large MUs are activated at low current intensity. As a consequence, all MUs can be simultaneously activated by the same pattern of activity. Secondly, high levels of activity can be imposed on the target muscle by electrical stimulation from the beginning, because the central nervous system, cardiovascular system, and other systems will not interfere with and limit the amount of activity, as is the case in exercise.27
In our non-randomized controlled trial, all dynamometric measurement results of both quadriceps femoris and tibialis anterior muscles in 3rd and 30th sec showed us that MS patients\\\', who were treated with HVPGS, muscle strength increased significantly. Additionally, for EMG and dynamometric measurement results of right QF, it was thought that important differences were because of the significantly higher values in the HVPGS group and the increased values in the right QF and TA muscles in the HVPGS group after the treatment. Meanwhile, MS patients\\\' fatigue was related with peripheral factors. Furthermore, significant differences were recorded between the treatment groups for mnf and mdf values of right QF muscle. QF is a big muscle recruited mostly with Type II fibers. The significant difference between the treatment groups proving that, MS patients who were treated with HVPGS recruited their type II MUs more than the MS patients in control (PNF) group. Meanwhile, we could not find similar difference for the left side QF, this may be because of the dominance and more usage of right side. Additionally, we thought that TA muscle was recruited mostly with Type I fibers, so may be HVPGS and PNF has the same affect in increasing the Type I fibers. There were no differences between the groups for TA muscle of both sides.
When we take into account these results, we concluded that after the treatment the values were occasionally increased because of the improvement in the strength in TA. The improvements in QF were may be because of the decrement of spasticity in QF in relation with treatment of weak knee flexors. While, after the treatment the results were more in HVPGS\\\'s favour, it was thought that HVPGS and PNF were not superior to each other. And in the light of these results, we made a decision as both HVPGS and PNF applications can significantly increase the strength of the muscles in MS patients. As our third main result, we concluded that with these physiotherapy and rehabilitation techniques, peripheral fatigue could be improved by changing the distribution and type of the fibers of the muscle and aerobic capacity.
Although we tried to do the necessary assessments and statistical analysis in accordance with the literature, our study has got limitations. We had seen that the area under the strength-duration curve was being used in the literature concerning power spectrum analysis, recently. These fatigue indexes may be more reliable, but they needed some special computer programs and can be used for future studies. Additionally, we could continue randomization with flipping coin method because of limited number of MS patients. To plan a rehabilitation programme with HVPGS, PNF and combination of them, further research could be organized with more MS patients and randomization could be done with block method.
Conclusion
With this non-randomized controlled trial we founded that MS patients have both central and peripheral fatigue. We also obtained that both HVPGS and PNF techniques have got almost similar effects on increasing the strength and decreasing the fatigue level.
While giving the absolute results was difficult, we found that HVPGS was more advantageous than the PNF. According, to our results, to obtain more localized and intensive effects, HVPGS was more impressive than the PNF. Another important finding is PNF was more effective when we want to obtain more general effects. Specific therapeutic applications, like HVPGS, could be a part of physiotherapy and rehabilitation programmes for strengthening and improving the peripheral fatigue.
References
1.Ng AV, Kent-Braun JA. Quantitation of lower physical activity in persons with multiple sclerosis. Med Sci Sports Exerc 1996; 517-23.
2.Comi G, Leocani L, Rossi P, Colombo B. Physiopathology and treatment of fatigue in multiple sclerosis. J Neurol 2001; 248: 174-9.
3.Petajan JH, White AT. Recommendations for physical activity in patients with multiple sclerosis. Sports Med 1999; 27: 179-91.
4.Vucic S, Burke D, Kiernan MC. Fatigue in multiple sclerosis: mechanisms and management. Clin Neurophysiol 2010; 121: 809-17.
5.Sliwa JA. Neuromuscular rehabilitation and electrodiagnosis.1.Central neurologic disorders. Arch Phys Med Rehabil 2000; 81: S 3-12.
6.de Haan A, Ruiter CJ, Van Der Woude LH, Jongen PJ. Contractile properties and fatigue of quadriceps muscles in multiple sclerosis. Muscle Nerve 2000; 23: 1534-41.
7.Balogun JA, Onilari OO, Akeju OA, Marzauk DK. High voltage electrical stimulation in the augmentation of muscle strength: effects of pulse frequency. Arch Phys Med Rehabil 1993; 74: 910-6.
8.Voss DE, Ionta MK, Myers BJ. Proprioceptive Neuromuscular Facilitation (third edition), Voss DE, Ionta MK, Myers BJ (Eds), Philadelphia: Harper&Row Publishers; pp vii-ix, 1985.
9.Wingerchuk DM, Noseworthy JH, Weinshenker BG. Clinical outcome measures and rating scales in multiple sclerosis trials. Mayo Clin Proc 1997; 72: 1070-9.
10.Schwid SR, Covington M, Segal BM, Goodman AD. Fatigue in multiple sclerosis: Current understanding and future directions. J Rehabil Res Dev 2002; 39: 211-4.
11.Schwid SR, Thornton CA, Pandya S, Manzur KL, Sanjak M, Petrie MD, et al. Quantitative assessment of motor fatigue and strength in MS. Neurology 1999; 53: 743-50.
12.Surakka J, Romberg A, Ruutiainen J, Virtanen A, Aunola S, Maentaka K. Assessment of muscle strength and motor fatigue with a knee dynamometer in subjects with multiple sclerosis: a new fatigue index. Clin Rehabil 2004; 18: 652-9.
13.Marthur S, Eng JJ, MacIntyre DL. Reliability of surface EMG during sustained contractions of the quadriceps. J Electromyogr Kinesiol 2005; 15: 102-10.
14.Ravier P, Buttelli O, Jennane R, Couratier P. An EMG fractal indicator having different sensitivities to changes in force and muscle fatigue during voluntary static muscle contractions. J Electromyogr Kinesiol 2005; 15: 210-21.
15.Allison GT, Fujiwara T. The relationship between EMG median frequency and low frequency band amplitude changes at different levels of muscle capacity. Clin Biomech (Bristol Aron) 2002; 17: 464-9.
16.Henze T, Rieckmann P, Toyka KV; (Multiple Sclerosis Therapy Consensus Group of the German Sclerosis Society). Symptomatic treatment of multiple sclerosis. Eur Neurol 2006; 56: 78-105.
17.Kesselring J, Beer S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol 2005; 4: 643-52.
18.Di Fabio RP, Soderberg J, Choi T, Hansen CR, Schapiro RT. Extended outpatient rehabilitation: its influence on symptom frequency, fatigue and functional status for persons with progressive multiple sclerosis. Arch Phys Med Rehabil 1998; 79: 141-5.
19.Baker NA, Tickle-Degnen L. The effectiveness of physical, psychological and functional interventions in treating clients with multiple sclerosis: a meta analysis. Am J Occup Ther 2001; 55: 324-31.
20.Kraft GH. Rehabilitation still the only way to improve function in multiple sclerosis. Lancet 1999; 354: 2016-7.
21.Sharrack B, Hughes RAC, Soudain S, Dunn G. The psychometric properties of clinical rating scales used in multiple sclerosis. Brain 1999; 122: 141-59.
22.Svensson B, Gerdle B, Elert J. Endurance training in patients with multiple sclerosis: Five case studies. Phys Ther 1994; 74: 1017-26.
23.Strimpakos N, Georgios G, Eleni K, Vasilios K, Jacqueline O. Issues in relation to the repeatability of and correlation between EMG and Borg scale assessments of neck muscle fatigue. J Electromyogr Kinesiol 2005; 15: 452-65.
24.Rasova K, Krasensky J, Havrdova E, Obenberger J, Seidel Z, Dolezal O, et al. Is it possible to actively and purposely make use of plasticity and adaptability in the neurorehabilitation treatment of multiple sclerosis patients? A pilot Project. Clin Rehabil 2005; 19: 170-81.
25.Rasova K, Havrdova E, Brandejsky P, Zalisova M, Foubikova B, Martinkova P. Comparison of the influence of different rehabilitation programmes on clinical, spirometric and spiroergometric parameters in patients with multiple sclerosis. Mult Scler 2006; 12: 227-34.
26.Rousseaux M, Perennou D. Comfort care in severely disabled multiple sclerosis patients. J Neurol Sci 2004; 222: 39-48.
27.Pette D, Vrbova G. What does chronic electrical stimulation teach us?. Muscle Nerve 1999; 22: 666-77.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: