
T. Chawla ( Departments of Surgery, The Aga Khan University Hospital, Karachi. )
G.N. Kakepoto ( Departments of Pathology, The Aga Khan University Hospital, Karachi. )
M.A. Khan ( Departments of Anesthesia, The Aga Khan University Hospital, Karachi. )
July 2001, Volume 51, Issue 7
Original Article
Abstract
Objective: In the absence of an explicit maximum blood order policy, ordering for blood transfusion is frequently based on subjective anticipation of blood loss instead of evidence based estimates of average requirement in a particular procedure. This study was done to assess current practice and the feasibility of a prospective randomized work to develop practice guidelines.
Method: We audited transfusion data for elective surgical procedures in our hospital during the last 2 years. Cross-matched to transfused ratio (CIT ratio) and Transfusion Index (Ti) for each of the elective surgical procedures was performed during the study period. CIT ratio is used as a measure of the efficiency of blood ordering practice14. It should ideally be between 2 and 2.5. We compared our results with the ideal.
Results: Data was analyzed for 32 elective surgical procedures in 2131 patients . Majority (2079) (97.56%) of the patients had CIT ratios higher than 2.5. Only 12 in 450 (21.11%) patients, had a Transfusion Index (Ti) higher than 0.5. There were 13 procedures in which both C/T ratio was greater than 2.5 and Ti less than or equal to 0.5.
Conclusion: In vast majority of elective surgical procedures routine cross match is not necessary. We propose a draft Maximum Surgical Blood Ordering Schedule (MSBOS). It provides guidelines for frequently performed elective surgical procedures by recommending the maximum number of units of blood to be cross-matched preoperatively. Implementation of MSBOS will result in about 60% reduction of cost to the patients (JPMA 51:2512001).
Introduction
Injudicious preoperative over ordering of blood can burden the physical and human resources of a health care facility and increase the cost of medical care.
In the absence of an explicit maximum blood order policy, ordering for blood transfusion is frequently based on subjective anticipation of blood loss instead of evidence based estimates of average requirement in a particular procedure5,6. Such practices have greater implications in resource-constrained settings. Data from several developing countries have shown gross over ordering of blood in 40% to 70% of patients transfused7-10.
The ratio between blood cross matching and transfusion (CIT ratio) should ideally be between 2 and 2.5. This means that at least 30% of the cross-matched blood should have been needed for transfusion. Any figure less than this is not justified.
A Maximum Surgical Blood Order Schedule (MSBOS) provides guidelines for frequently performed elective surgical procedures by recommending the maximum number of units of blood to be cross-matched preoperatively11. A MSBOS reduces the preoperative cross matching of blood in surgical cases in which there is less likelihood of blood transfusion1,2. Implementation of MSBOS has almost universally resulted in substantial reduction of direct and indirect costs12. It has also proven to be an effective tool for quality assurance by reducing the stress on the blood transfusion services, more efficient use of bloodstocks and reduction in the wastage due to outdating.
As a first step towards developing a Maximum Surgical Blood Order Schedule for The Aga Khan University Hospital, we conducted a retrospective study of different surgical services to find out the current transfusion practices. The CIT ratio, Transfusion Index (Ti) and possible cost savings for various commonly performed elective surgical procedures was also assessed.
Methods
The transfusion data for elective surgical procedures for the period between July 1998 and June 2000 was analyzed. The medical record numbers of the patients undergoing elective surgical procedures were taken from the coded record and the data for cross-matched units and actual transfused units was retrieved from the Blood Bank database. The two data sets were merged using Admission Number as the unique primary key. Currently The Aga Khan University Hospital Indexing and Coding department codes all surgical procedures based on ICD-9 classification. We modified these codes to develop surgical procedure categories for the purpose of this study. Data was analyzed for procedures with a minimum of 5 cases in the study period.
The cross-matched to transfused ratio (CIT ratio) and Transfusion Index (Ti) for each of the elective surgical procedures performed during the study period was calculated. CIT ratio is used as a measure of the efficiency of blood ordering practice.2,13-16. A ratio of more than 2.5 indicates excessive cross matching of blood for a specific procedure. Transfusion Index is defined as the average number of units transfused for a given procedure. Ti of more than 0.5 indicates that blood needs to be cross-matched preoperatively for that procedure9. However, Ti has a potential of being influenced by occasional large transfusions
Mead’s criterion2,15 (average units used for a procedure x 1.5) was used as a guide to recommend the number of blood units, which need to be cross-matched preoperatively for each procedure.
Mean Direct Multiple Cost to the patient was defined as the Rupee amount paid by the patient on blood cross-match and transfusion for each procedure and then the direct multiple cost per case for each surgical procedure was calculated for the study period. The direct cost per case was also calculated that would have been paid by the patient if a Maximum Blood Ordering Schedule were in place. The latter was subtracted from the former to calculate possible direct savings for the patient. Statistical analysis was performed using SPSS© for Windows. Currently.
Results
Data was analyzed for 32 elective surgical procedures in 213 1 patients (Table 1).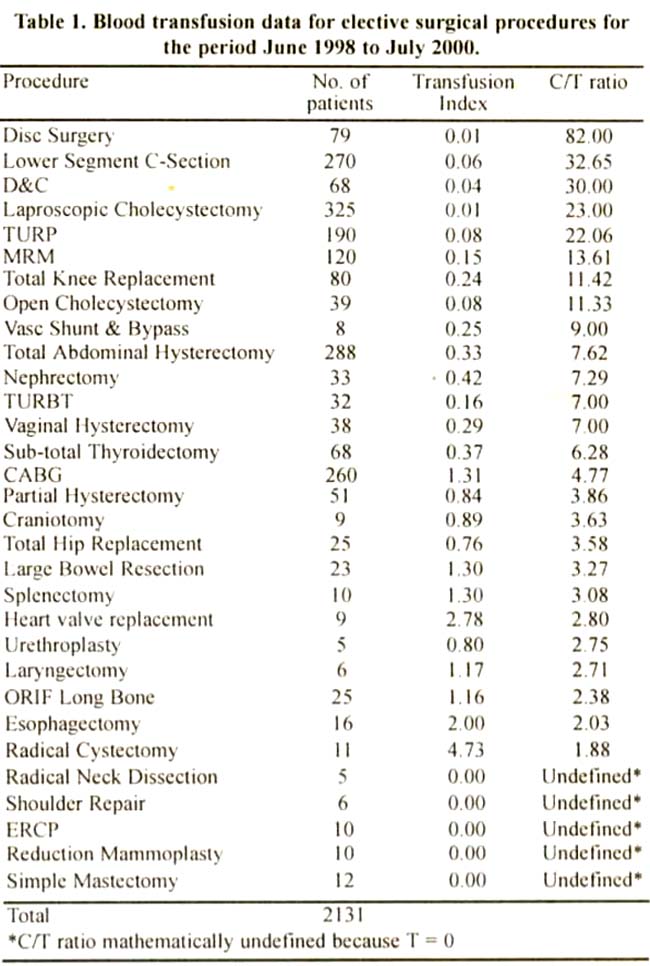
Twenty-three of these procedures, in 2079 (97.56%) patients, had CIT ratios higher than 2.5. The procedures with the three highest mean C:T ratios were Disc Surgery (CIT ratio 82). Lower Segment Caesarian Section (C/T ratio 32.65) and Dilatation and Curettage (CIT ratio 30.00). Only twelve procedures in 450 (21.11%) patients, had a Transfusion Index (Ti) higher than 0.5. There were thirteen procedures in which both CIT ratio was greater than 2.5 and Ti less than or equal to 0.5.
The charge to the patient for the first unit of packed cells cross-matched at AKUH Blood Bank is Rs 860. The charge for every subsequent unit cross-matched is Rs 800. If no transfusion is given, the patient charge of Rs 300 per unit is retained and the rest is refunded. The charge of ABO grouping and antibody screening (G and S) is Rs 460 and this test is only done once on the patient’s sample for every surgical procedure.
The mean direct multiple costs per case ranged between Rs. 5036 for Radical Cystectomy to Rs. 600 for ERCP, Reduction Mammoplasty and Shoulder Repair (Table 2).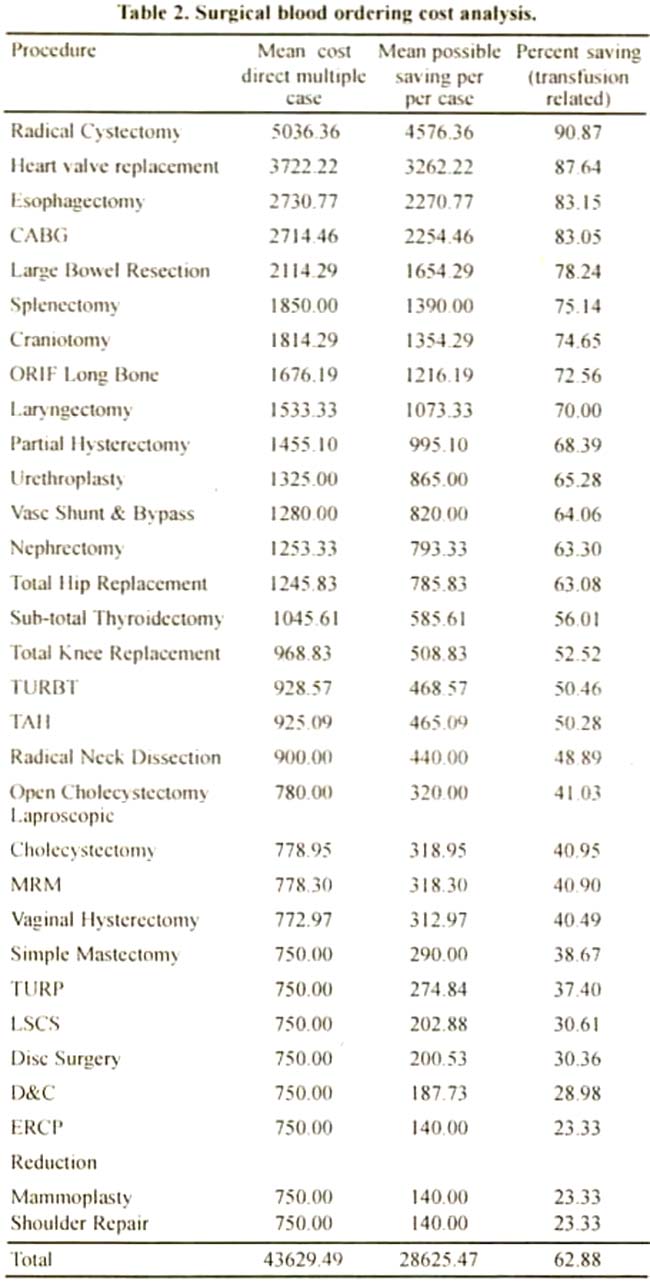
The possible direct savings, if an MBOS were in place, ranged between from 90.87% to 23.33%. The overall mean possible direct savings were 62.88%.
Discussion
These results show that in the absence of a Maximum Blood Ordering Schedule, there is a high resulting in additional costs to the patient. These findings highlight the need for a Maximum Blood Ordering Schedule. It was also shown that implementation of an MSBOS will result in approximately 60% reduction of cost to the patient. High savings have also been reported in the literature8. Implementation of MSBOS will also decrease the opportunity cost of holding blood ‘out of circulation’ for patients who may not require transfusion and better management of stocks.
We recommend that the procedures with Transl’usion Index less than or equal to 0.5 should not have a routine cross-match (antiglobulin): instead the sample which is sent to the blood bank well in advance, preferably one day before surgery, should have ABO grouping and antibody screening after grouping has been done (G and S). if the antibodies are negative this should suffice. if transfusion is required on the day of surgery , very occasionally in such pat ients, then a “rapid spin cross-match” with blood of the same ABO and Rh D group should be preformed. This requires very little time (5 to 10 minutes) if antibodies are already known to be negative and the packed cell unit can be released immediately if found compatible. On the other hand if antibodies are found to be positive during initial ABO screening, then it is suggested that a complete antiglobulin cross-match is done at the time of the screening to find a compatible unit. The system should have flexibility for individual patients in whom clinical circumstances indicate potential requirement of blood beyond Ti. In such cases, extra units may be cross-matched. However the frequency of transgressing recommended policy should be monitored to prevent abuse of the system.
Many hospitals in the developed countries have adopted the policy of using G and S instead of cross-match for a proportion of surgical procedures. This technique has proven to be effective without compromising patient safety9-12,14 In some countries even the rapid spin cross-match is not done if no red cell antibodies are present in patient’s serum. ABO and RhD compatible blood is cross-matched electronically using computers and released for transfus ion.
It is important to recognize that effective implementation of such policy is dependent not only on the cooperation of all surgical specialties but also of other related entities e.g. anesthesia, blood bank etc. Surgeons, anesthetists and other users may not be confident about the availability of blood in time if MSBOS is implemented. Hematologist should take users in confidence and explain to them very clearly about the operation of MSBOS. It should be explained to the users that should there be an emergency, compatible blood can be provided within 5-7 minutes after doing a 2-5 minutes rapid spin cross-match.
Based on the analysis of retrospective data, we have developed a draft Maximum Blood Ordering Schedule for AKUH (Appendix A).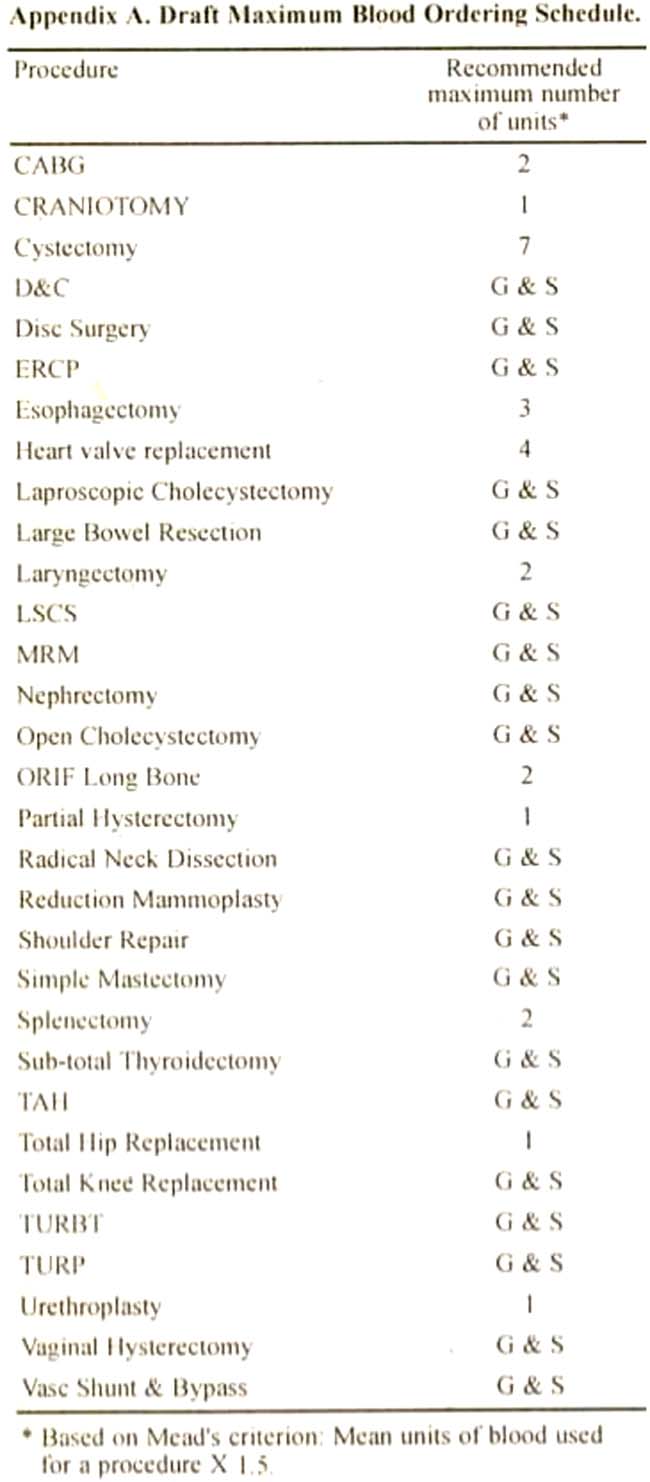
it is recommended that MBOS should be revised yearly on the basis of the latest available data to keep it responsive to the changing needs of the hospital.
References
1.Sinaliwood JA. Use of blood in clectivc general surgery: an area of wasted resources. Br Med. J., (Clin Res Ed). 1983:286:868-70.
2.Seshadri RS, Odell WR, Roxhy D, et al, EfFective use of blood in elective surgical procedures. Med J, Aust., 1979,2575-578.
3.Vibhute M, Karnath SK. Shetty A, Blood utilization in elective general surgery cases: requirements, ordering and transfusion practices. J. Postgrad. Med., 2000 46:13-7.
4.Bhutia SG, Srinivasan K, Ananthakrishnan N. Blood uiiliiation in elective surgery--requirements, ordering and transfusion practices. Nat Med. J. India., 1997:10:164-8.
5.Lim EJ, Lopez CG, Veera SN, et al. Efficiency of blood usage for elective surgery in the University Hospital Kuala Lumpur. Malays J. l’athol., 1996:18:107-12.
6.Juma 1, Baraka A, Abu-Lisan M, et at. Blood ordering habits for elective surgery: time for chaitge. J. R. Soc. Med., 1990:83,368-70.
7.Lowery TA, Clark JA, Successful implementation of Maximum Surgical Blood Order Schedule. J Med Assoc, Ga., 1989:78 155-8.
8.H ardy NM, Bolen FH, Shatney CH Maximum surgical blood order schedule reduces hospital costs. Am. Surg., 1987:53:223-5.
9.Mintz PD, Lauenstein K, Hume J, Henry Bli, Expected Hemotherapy in elective surgery. JAMA 1987. 239:623-5.
10.Mead 3, Anthony CD, Saltier M. Hemotherapv in elective surgery. An incident report, Review of literature and alternative for guideline appraisal. Am. J. clin Path., 1980:74:221-7
11.Friedman BA. An analysis of surgical blood use in United States. Hospital with application of the maximum blood surgical blood order schedule. Transfusion 1979:19:268-78.
12.Napier JAF, Biffin All, L .av D. Efficiency of use of blood for surgery in south and mid Wales. Br. Med. .J., 1985, 291 799-801
13.Argov S, Shechter Y. is routine cross matchaing for two units of blood necessary in elective surgery2 Am. J. Surg., 1981:142:370-1.
14.Boral LI, Dannamiller FJ. Stanford W, et al. A guideline for anticipated blood usage during elective surgical procedures. Am. J. Clin Pathol,, 1979;71:680. 4.
15.Pathi VL, Goshi S. Cuscheri A. Its Scotland’s blood, so why waste it’! J. R CoIl. Surg. Edinb., 1987:32:69-71.
16.Lee K. Lachanee V. Type and screen for elective surgery. Result in one vear experience in a small community hospital. transfusion . 1 980,20 324-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: