
Ghous Bukhsh Soomro ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
Zaigham Abbas ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
Mujahid Hassan ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
Nasir Luck ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
Yousuf Memon ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
Abdaal Wasim Khan ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi. )
March 2011, Volume 61, Issue 3
Short Reports
Abstract
The objective of this study was to find any association of extrahepatic biliary atresia (EHBA) with a possible infectious etiology. Infants diagnosed to have EHBA were tested by blood PCR for cytomegalovirus (CMV ), Ebstein-Barr virus, HBsAg, anti-HCV and IgM antibodies for CMV, toxoplasma, rubella, and herpes infections. Thirty-three infants of EHBA were included in the study, male 22, median age when diagnosed 2.5 months (range 1.0-5.0 months). On examination pallor, oedema and hepatosplenomegaly were seen in all and ascites and microcephaly in 19 (57.6%). Centile height and weight were 50th in 23 and 25th in 10. Persistent CMV infection documented by PCR was present in 14 (42%) patients. Eleven of these also had positive CMV IgM antibodies. No other above mentioned infections could be detected in our patients of EHBA. Our data suggests that CMV infection may play a role in the pathogenesis and progression of EHBA.
Keywords: Extrahepatic biliary atresia, Cytomegatovirus, PCR.
Introduction
Extrahepatic biliary atresia (EHBA) is an important cause of neonatal cholestatic jaundice. The disappearing bile ducts are thought to be a result of destructive inflammatory process which starts in the perinatal period.1 The etiology of biliary atresia is poorly understood. This extrahepatic obstructive cholangiopathy is progressive after birth resulting in worsening neonatal cholestasis, eventually leading to secondary biliary cirrhosis and liver failure.2 The process seems to be an acquired one. There is controversy about the etiological role of viruses. The studies have implicated reoviruses, rotaviruses and cytomegalovirus (CMV).2 The objective of this study was to find out any association of extrahepatic biliary atresia (EHBA) with exposure to TORCH infections (toxoplasma, rubella, cytomegalovirus (CMV), herpes simplex virus and Ebstein-Barr virus (EBV), hepatitis B and C.
Methods and Results
Infants presenting with cholestatic jaundice were evaluated for the presence of biliary atresia. Abdominal ultrasound and radionuclide cholescintigraphy using technetium-labeled diisopropyl iminodiacetic acid were performed in each case . Diagnosis of EHBA was made by absence of gallbladder and no biliary dilatation on ultrasound and . failure of excretion of radiolabel on nuclear scintiscan. confirmed the presence of EHBA.
The infants diagnosed to have EHBA were further evaluated by full history taken from parents and complete physical examination. Laboratory investigations included complete blood counts, liver function tests, clotting profile, blood cultures, and presence of toxoplasma, rubella, CMV and EBV infection and hepatotropic viruses. Tests performed for this purpose included blood PCR for CMV and Epstein Bar Virus (EBV), IgM antibodies for CMV, toxoplasma, rubella, and herpes infections, HBsAg and anti-HCV antibody. All the immunological tests were performed by Chemiluminescence Microparticle Immuno Assay (CMIA) by the clinical laboratory of the hospital. Liver biopsy could be performed in 25 patients after correcting the coagulation abnormalies.
Thirty three infants of EHBA were included in the study; male 22, median age of diagnosis 2.5 months (range 1.0-5.0 months).Median birth weight 2.9 kg (2.5-3.2), median gestational age 39 weeks (38-40). These patients presented with jaundice, clay coloured stools, diarrhoea, and poor feeding. Thirty two (97%) were febrile and 31 (93.9%) were having pruritis. On examination pallor, oedema, hepatosplenomegaly and ascites were present in all patients. Microcephaly was noticed in 19 (57.6%). No other dysmorphic features were present. At the time of presentation, centile height and weight on CDC growth charts3 were 50th in 23 and 25th in 10. Results of the laboratory tests have been mentioned in Table-1.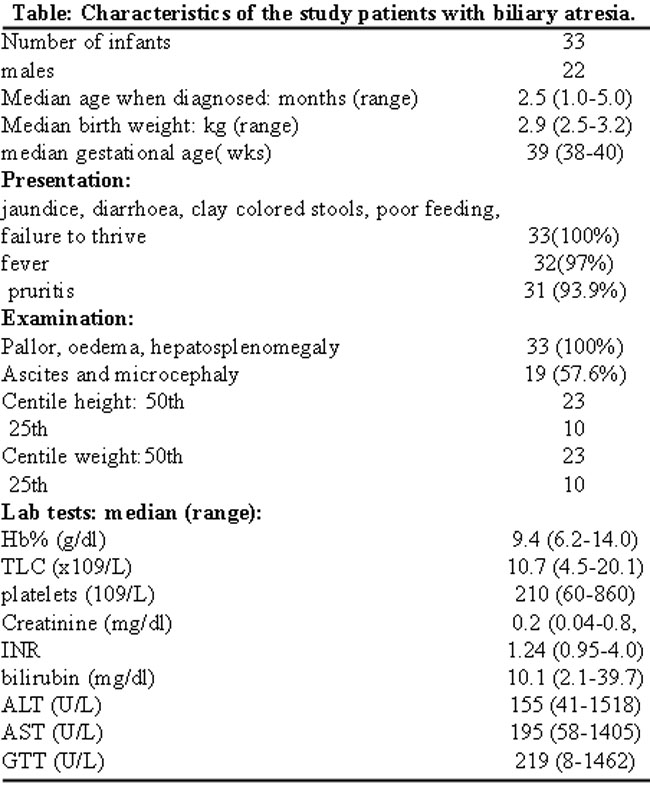
Liver biopsy done in 25 patients was suggestive of established biliary cirrhosis in all cases. Twenty-one patients had already underdone Kasai\\\'s portoenterostomy at the time of presentation.
Persistent CMV infection as detected by blood PCR was present in 14 (42%) patients. Eleven (33.3%) of these also had positive CMV IgM antibodies. No other TORCH infection i.e. toxoplasma, rubella , or herpes simplex could be detected in our patients of EHBA. PCR for EBV virus, HBsAg and anti-HCV were also negative.
Conclusion
Biliary atresia is the most frequent indication for liver transplantation in children. Portoenterostomy is the only available treatment, with better results when performed in the first two months of life.4 Transplantation has been suggested as the initial procedure of choice because of its excellent long-term survival rate and the fact that more than 60% of infants undergoing the Kasai procedure ultimately require liver transplant mention.5
The etiology of EHBA is not fully understood. The inflammatory response in the livers of these patients mimics that observed during viral infections. Portal bile ductular proliferation, bile plugging, portal-portal fibrosis, and an acute inflammatory reaction are characteristic findings in infants with biliary atresia.6 There is a possibility of primary perinatal hepatobiliary viral infection generating a secondary autoimmune-mediated bile duct injury. One study demonstrated CMV IgM immunoglobulin deposits on the hepatocellular canalicular membrane in infants with CMV infection.7 In patients with biliary atresia and cytomegalovirus infection, liver fibrosis seems to be more severe with a lower rate of jaundice disappearance after Kasai procedure and a higher post-operational reflux cholangitis.8
CMV is known to cause intrahepatic cholestasis in infants and responds to the treatment.9 Our study indicates possible association with EHBA as well. It is important to recognize this as early treatment of CMV may suppress the immune mediated response, decreasing the inflammatory damage to bile ducts. It may delay the need for liver transplantation. Most of our patients were referred cases who were sent back to their physicians. They had already developed cirrhosis. Treatment outcome could not be assessed in these patients. There is low accuracy of serological tests for detecting active CMV infection as compared to PCR done on liver tissue.10 Though CMV infection could be documented only in one third of our patients by blood PCR, the frequency might have been higher if we had done PCR on liver biopsy samples. Our data suggests an association of EHBA with CMV infection which may play a role in the pathogenesis and progression of EHBA.
References
1.McKiernan PJ, Baker AJ, Kelly DA. The frequency and outcome of biliary atresia in the UK and Ireland. Lancet 2000; 355: 25-9.
2.de Carvalho E, Ivantes CAP, Bezerra JA. Extrahepatic biliary atresia: current concepts and future directions. J Pediatr (Rio J) 2007; 83: 105-20.
3.Clinical growth charts. Centres for disease control and prevention, USA. (Online) (Cited 2010 Sept 16). Available from URL: http://www.cdc.gov/growthcharts.
4.Sanghai SR, Shah I, Bhatnagar S, Murthy A. Incidence and prognostic factors associated with biliary atresia in western India. Ann Hepatol 2009; 8: 120-2.
5.Otte JB, de Ville de Goyet J, Reding R, Hausleithner V, Sokal E, Chardot C, et al. Sequential treatment of biliary atresia with Kasai portoenterostomy and liver transplantation: a review. Hepatology 1994; 20: 41S-48S.
6.Qureshi MA, Shaukat M. Biliary Atresia: Liver histology and its` relation to the age of the patient. Pak Paed J 2006; 30: 193-6.
7.Fischler B, Woxenius S, Nemeth A, Papadogiannakis N. Immunoglobulin deposits in liver tissue from infants with biliary atresia and the correlation to cytomegalovirus infection. J Pediatr Surg 2005; 40: 541-6.
8.Shen C, Zheng S, Wang W, Xiao XM. Relationship between prognosis of biliary atresia and infection of cytomegalovirus. World J Pediatr 2008; 4: 123-6.
9.Tezer H, Seçmeer G, Kara A, Ceyhan M, Cengiz AB, Devrim I, et al. Cytomegalovirus hepatitis and ganciclovir treatment in immunocompetent children. Turk J Pediatr 2008; 50: 228-34.
10.Oliveira NL, Kanawaty FR, Costa SC, Hessel G. Infection by cytomegalovirus in patients with neonatal cholestasis. Arq Gastroenterol 2002; 39: 132-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: