
R. Liefooghe ( VLIR project, Sialkot, Islamabad. )
A. D. Muynck ( HAS-SHAIP, Islamabad. )
January 2001, Volume 51, Issue 1
Original Article
Abstract
Aims: To establish various factors that affect TB treatment adherence over time.
Design/Setting: Semi-structured questionnaire. All newly diagnosed cases of TB at Bethamia Hospital, Sialkot were interviewed at the beginning of treatment, one month of therapy and at the end of intensive phase. Results: Perception of TB as a stigmatising disease was found related to early defaulting and to a lesser degree to late defaulting. Knowledge of TB in itself did not have a clear impact on defaulting, but the attitude towards interruption of treatment did. The strongest risk factor is irregularity of dt’ug intake and appointment keeping.
Conclusion: Strategies to improve treatment adherence should concentrate on methods to iticrease patient’s motivation for treatment (JPMA 51:3; 2001).
Introduction
Low adherence to the treatment regimen has been recognized as a major threat for tuberculosis (TB) control program1. A successful treatment plan consists of the daily intake of a combination of drugs for a period of 6 to 9 months. TB patients obviously face many constraints in order to adhere to this treatment. To gain a better understanding of the process of treatment adherence it is necessary to identify its determination factors and especially those that are vulnerable to change. The majority of studies have concentrated on socio economic factors such as age, gender, education, occupation, travel distance or knowledge of TB2-5. Other important behavioural factors described in more recent health behaviour models6,7 such as intention to comply; perceived barriers to TB treatment; attitudes towards the treatment and social support, are often overlooked. TB is a major cause of ill health in Pakistan8. Several studies documented the problem of low treatment adherence9-11. Others have shown that behavioural factors12, including social stigma13, contribute to non-adherence.
This study was carried out in Bethania Hospital (BH), Sialkot. Annually, approximately 1000 TB patients receive treatment in BH14. Newly diagnosed sputum positive cases receive daily four drugs during the intensive phase (2 months) followed by two drugs daily for the continuation phase (6 nionths)1. To ensure treatment supervision during the intensive phase, hospitalisation was recommended for all sputum positive cases. The study amied to understand the barriers and problem areas in TB treatment compliance. An attempt was made to identify the dynamics of the risk factors in the intensive and continuation phases of treatment.
Patients and Methods
Risk factors for defaulting were assessed through semi-structured interviews. For each patient information was collected at the start of the treatment (T0), after one-month (T1) and at the end of the intensive phase (T2). Questions were based on previous qualitative13,15 and quantitative studies16. Questionnaires were pretested and adapted where necessary. All participants gave their informed oral consent voluntarily.
Variables Measured
Intention to comply was measured by the question “Are you confident you will finish the entire treatment” and recorded on a 1-5-point scale(T0-T1-T2)11. Perceived barriers were measured at different points in time (T0-T1T2). To assess the attitude towards the curability of TB, patients were asked to give their opinion on six statements on a 1-5-point scale (T0-T1-T2). Perceived stigmatisation score was measured by the sum of patient’s agreement on seven statements (T0-T2).
Subjective social control was measured through two questions on a 1-5-point scale. Patients were first asked to what extent they believed their family, relatives or friends were convinced that they should comply with the TB treatmand secondly how strongly this opinion would affect their own decision to comply (T0-T1-T2).
Social support was assessed by several questions concerning the financial and material support (bringing food to the hospital, looking after the children, helping in the fields) given to the patient (T1-T2). For OPD patients, regular drug intake was assessed twice (T1-T7) by the question “Did you ever forget to take your drugs?”.
Regularity of the treatment: A regular patient was defined as a patient who was never more than 2 days late for a check-up appointment in the intensive or for more than 7 days in the continuation phase. Assessment of knowledge of TB consisted of questions concerning the transmission of TB (T0-T2) and the duration of treatment (T0-T1-T2). The attitude towards treatment adherence was measured by askiiig patients to indicate their agreement, on a 5 point scale, with the statement: “Do you believe that stopping your treatment before completing the full course will be harmless or harmful to your health?” (T1-T2).
Demographic profile included age, gender, tehsil of residence and marital status. Socio-economic status was measured by schooling (none, primary, or higher); #persons in the family; dependency ratio (#persons in the family! #persons economically active), occupation and whether the patient was the sole breadwinner). The outcome parameter was defaulting. A defaulter was defined as a patient who interrupted treatment for more than two consecutive months. Patients who defaulted in the intensive treatment phase were defined as “early defaulters"; those who defaulted during the continuation treatment phase as “late defaulter”.
Data Analysis
Data were analysed by SPSS-plus software. Risk factors of patients’ defaulting were assessed in two strata:
the intensive phase and the continuation phase for those who had completed the inteiisive phase. The relative risk of defaulting was used as the parameter of association; the alpha error was put at a 0.05 level. Throughout the study, bilateral hypotheses were tested. The association were tested through t-test for equality of means, X2 test of association and X2 test of linear trend; 95% confidence intervals (CI) around the rate ratios (RR,) are given.
Results
Study Population
Six hundred and fill three sputum positive TB cases were diagnosed between September 1996 and October 1997 at BH. The criteria for eligibility was that the patients had to be 15 years or older, not critically ill and the follow-up to the treatment carried out in BH. Patients who died (47) or were transferred out (15) or failures (8) were eliminated from the study. Fourteen initial interviews were missed (2.5%) and 3 patients refused to be interviewed, the remaining 563 patients constitute the study population.
Of 563 patients 44% were females and 56% males. More than 70% of the patients were between 15-45 years. The educational level was very low; half of the patients had not received any form of education. This was even more so for women of whom only one third had had any schooling at all. The majority (73%) of patients were residents of Sialkot district. Almost all patients (90%) accepted hospital admission initially but only 54% completed the full two months of supervised treatment in the hospital. Overall 433 (77%) complied with the entire treatment course and 130 (23%) defaulted.
Defaulters in intensive treatment phase (Early defaulters)
Sixty patients defaulted during the intensive treatment phase. They were somewhat older (35.5 vs. 30.0 years median age) than compliant patients and contained 1.5 times more males than females. Patients living outside Sialkot district defaulted two times more than those living in the district did (RR=2.3: Cl: 1.5; 3.7). Illiterate patients had a higher risk of defaulting (RR=1.8; Cl: 1.1; 3.0) compared to literate patients. Single patients had half the defaulter rate (6.1%) than married patients (12.6%), while those widowed, separated or divorced had the highest rate (14.3%). No significant differences were found for other socio-economic indicators.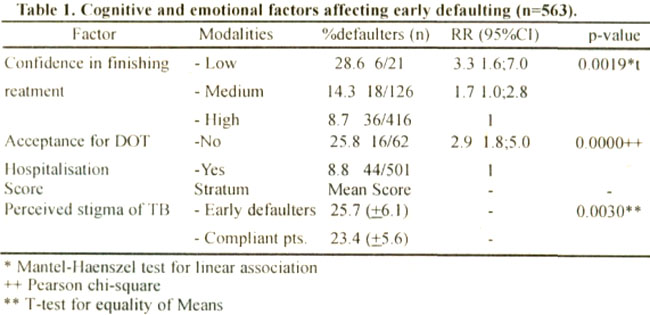
Table 1 summarises factors significantly aftecting early defaulting. At the start of treatment, three quarters of the patients felt very confident they would finish the entire treatment course. Those who expressed less confidence in their ability to conform to the treatment requirements had a higher risk of early defaulting. Low confidence was related to a lower belief in the curability of TB (P=0.024).
Early defaulter rates were three times higher in patients who rejected hospitalisatior.. They perceived more constraints (mean score 15.5 +5.0 vs 13.5 ±4.1; p=0.002) and had a more negative image of TB (stigmatisation score 25.2 ±6.6 vs 23.4 ±5.5 :p=0.02). Many patients perceived TB to be a stigmatising disease. The majority agreed that “one should avoid talking to others about one’s disease”. They clearly felt that their friends and relatives should not know they had TB. Half of them believed “113 has life long consequences” and a quarter felt “it is difficult to earn a living after recovering from TB”. Early defaulters felt stronger about the stigma. This was mainly because considerably more defaulters felt “TB in the family to be a disgrace” and “friends desert you when you have TB”. Initial knowledge of TB and ‘TB treatment did not differ significantly between defaulters and non-defaulters. Almost all patients were aware they had TB. Only one in three patients knew the correct duration of the treatment and only one out of four how TB is transmitted.
Defaulters anticipated more obstacles to the treatment than compliant patients did (Table 2).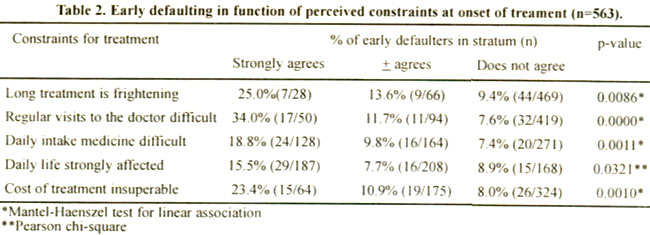
The regular visits to the doctor, long treatment and cost of the treatment were the most important constraints. A significantly negative correlation was observed between the motivation for the treatment and perceived barriers (rp=0.29: p<0.0001 )iii.
Second month defaulters
Thirty early defaulters were interviewed at T1, three inter-views were missed. Six interviews of compliant patients were also missed. After one month of treatment, almost all patients felt their health had improved. The few, who did not, had a seven times higher risk of defaulting in the following month (RR=7.2: 95% Cl: 3.0; 17.2). Low confidence in finishing the treatment quadrupled that risk (RR=4.0; 95% CI: 2.0; 8.0). In addition, patients who were not convinced of the harmful effects of discontinuing treatment had twice the risk of defaulting in the following month.
The importance of social support became evident during the second interview (Table 3).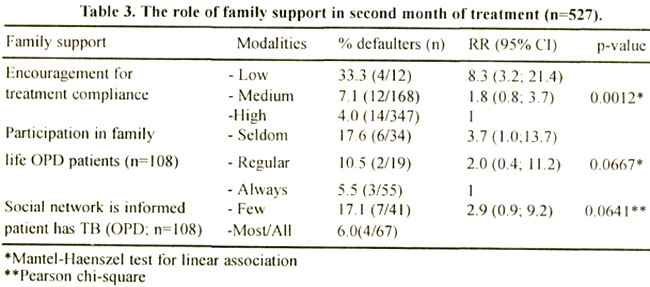
Less encouragement from the family for the daily drug intake or for the continuation of treatment, resulted in a higher risk for defaulting. For OPD patients, a link was observed between the degree of social isolation and defaulter rates. Not surprising, those who seldom participated in family life or whose friends ignored them, reported a higher stigma score (25,7+4. 6 vs 23.4±5.6). Equally, OPD patients who concealed their disease from their environment had three times the risk of defaulting compared to those who did not. Again, concealing the disease was linked to a significant stronger perception of stigmatisation ( mean score 26.0+5.5 vs 22.7+5.4).
Defaulting during the continuation phase (Late defaulters) Of the 503 patients who complied with the intensive treatment phase, 493 could be interviewed (12). Seventy patients defaulted in the continuation phase, 63 of these were interviewed (90%). Only three interviews (0,7%) were missed out of the 433 compliant patients.
More late defaulters had no or only primary schooling: lived outside the coverage area and had a longer history of illness (Table 4).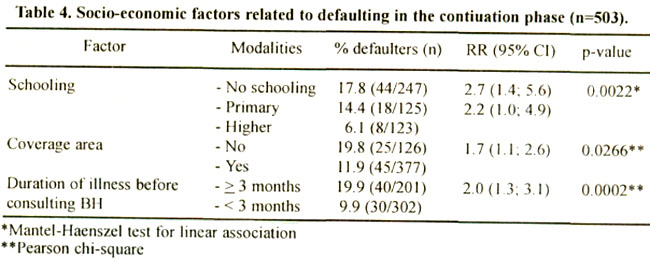
The relation between schooling and defaulting was stronger i n women than in men: illiterate women had a 3-1/2 times greater risk of defaulting than literate women (RR=3.4: Cl:1.2;9.5); for men this was only 1-1/2 times (RR=1.6:Cl:0.9; 2.7). Remarkbly, none of the higher educated females defaulted.
At this stage of the treatment, 99% of the patients were receiving strong encouragement from their family to comply with the full course. The financial support of the family became important in the continuation phase and patients who had no financial support had thrice the risk for defaulting (Table 5).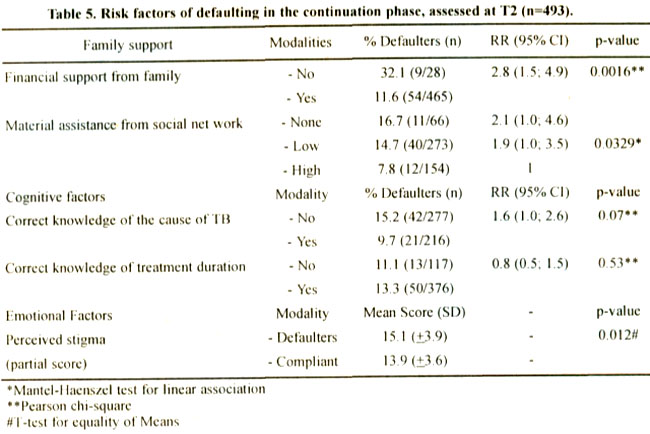
Material assistance from the social network such as regular visits from family and friends, assistance with the care of children, in the home, with the job or studies, contributed to compliance. After two months of treatment, basic knowledge of TB improved substantially. The number of patients that correctly stated the transmission mode of TB or the correct length of TB treatment doubled from 21% to 44% and from 35% to 74% respectively. The effect of knowledge on treatment adherence was rather negligible.
The perception on stigma related to TB had not drastically changed. Ninety percent of the TB patients still agreed that “you should not talk to others about your disease”, 51% believed “TB to be a disgrace to the family”. Late defaulters scored significantly higher on four statements. They feared that “even best friends might desert them because they had TB”. More agreed that TB patients should hide their disease for their family or for friends and believed that “TB patients will experience the consequences of the disease for the rest of their life”.
Correct drug intake and regularity of treatment strongly related to a better treatment adherence (Table 6).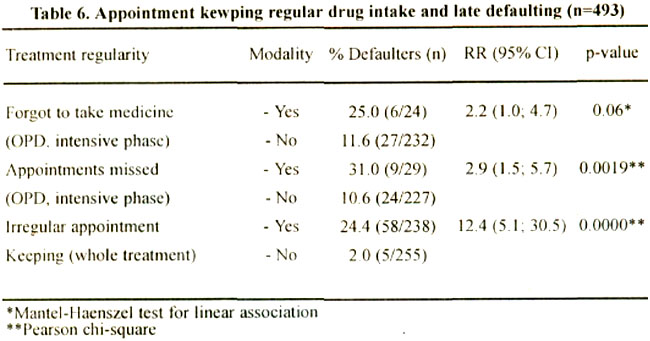
If during the first two months of treatment OPD patients forgot to take their medicine, they had twice the risk for defaulting. Those who were late for the scheduled appointment, even once, had 3-1/2 higher defaulter rates as those who attended regularly. The relationship became even stronger if appointment keeping during the whole treatment course is considered. In such cases, a patient who missed a single appointment had more than twelve times the risk of defaulting compared to patients who kept the scheduled dates.
Discussion
Different mechanisms influence treatment adherence behaviour over time. Motivation at the start of treatment is an important predictor for early defaulting. Lack of confidence in the capability to finish the full treatment course increases the likelihood for defaulting in the early weeks of treatment. Motivation is easy to assess at the start of the treatment through a simple question like “How confident are you that you will be able to finish the treatment course?” However, motivation has to be understood in the context of the constraints patients’ face in their every day life. The greater the anticipated barriers at the start of treatment, the higher the risk for early defaulting. Early defaulters are also more reluctant to accept the supervised treatment in hospital17.
The findings show that the family’s encouragement for the treatment is an essential element in the intensive phase. As treatment advances, financial support from the family becomes increasingly important. The financial burden of the TB treatment is difficult to overcome by the patient and his/her nuclear family alone. To be able to fulfil the treatment requirements patients often iieed practical assistance, such as help with the children, household, job or studies. Kinship institutions such as biraderi are central to the social life in Pakistan. They provide, through a network of kinship, a support mechanism. In case of illness, a person can count on the biraderi for moral, financial and practical support18. As found elsewhere19-21, for TB patients this support is extremely important and positively associated with an improved treatment adherence. Clearly, late defaulters receive less support from their social network. They also feel more stigmatised.
Stigmatisation is reflected in the negative perceptions patients have about the disease13,22. Even after two months of treatment, the majority of patients still conceal their health problem from their environment. Neither the interaction with the health care providers nor improvements in the patients’ condition could after the preconceived ideas of the social stigma.
Knowledge about transmission of TB and regimen duration is low at the start of treatment but improves over time. The study confirms that better knowledge does not influence treatment adherence23. However, a careless attitude towards prematurely stopping the treatment dose. Apparently imparting knowledge or an advice-giving approach is insufficient to motivate TB pat ients to adhere to the treatment. Efforts should rather focus on providing support and enabling patients to overcome treatment barriers.
One of the best predictors of adherence to the full treatment course is early compliance. Patients who forget to take their drugs or who are late for their appointments, even once, have a high risk of becoming defaulters. This corroborates the findings of a study carried out in Rawalpindi in which irregular appointment keeping was the strongest predictor for subsequent defaulting9. This factor is easy to assess and has a powerful operational value: patients who are from the start erratic in drug intake and appointment keeping will need extra support and guidance.
Socio-economic status is often mentioned as an important predictor for treatment adherence. We only found a slightly higher “early defaulter” rate in vulnerable groups such as widowed/separated patients. The predictive value of geographical accessibility is apparent. Regular treatment follow-up beyond a certain distance from the treatment centre seems to be very difficult. This problem can only be solved once a network of conveniently located TB treatment centres becomes available.
The relationship between education and treatment adherence has been established before2.24, For Pakistan, a country with a low female literacy rate25, it is important to report that in particular, female education has a strong potive impact on treatment adherence.
Classical economic factors such as occupation, dependency ratio or being the sole breadwinner are not related to treatment outcome. In the cultural context of the Pakistani “biraderi” support system, financial and material support from the network is probably a more meaningful soclo-economic indicator.
References
1.Ngamvithayapong-Yanai J. Petchawan P. Yanai II. Compliance to tuberculosis: A gentler perspective, in: Diwan VK, Thorson A and Winkvist (Eds), Gender and tuberculosis. N.Y.. The Nordic School of Public Health. 1998, pp.127-48.
2.Johansson E. Diwan VK, Iluong ND, et a!. Staff and patients attitude to tuberculosis and compliance with treatment: an exploratory study in a district in Vietnam. Tubercie. Lung l)is.. 1996: 77: 178-83.
3.Rideout M, Menzies R. Factors affecting compliance with prevcntive tuberculosis treatment. Clin Invest Med, 1994; 17: 31-36.
4.Reed JB, Mecausland R, Elwood JM. Default in the outpatient treatment of tuberculosis in two hospitals in Northern India. J. Epidemiol Community Health, 1990: 44: 20-23.
5.Sultan A A. Naseer A. Abid Parvez, A Compliance in tubercular patients at Faisalabad. Pak. J. Med. Res.. 1989; 28: 42-46.
6.Randura A. Social foundations of thought and action: A social cognitive theroy. Englewood Clifis. N.J. Printice-Ilall. 1986.
7.A;ieo I. From intentions to actions: A thoery of planned behaviour, In: .I, Kohl and j. I3eckman (Eds). Action—control: From cognition to behavior. Heidelberg. Springer, 1985. pp. 11-39.
8.Ilussain R, Toossi 7. Hasan R. et al. Immune response profile in patients with active tuberculosis in a BCG vaccinated area. Southeast Asian j. Trop. Med. Public Health, 1997; 28: 764-63.
9.Dc Muynck A. Khan II. Awan M. et al. Gender and Tuberculosis: a control at district level. HSA Monograph 2, 1999, pp. 102-112. retrospective cohort study at TB Center. Rawalpindi. In: De Muynck A., Siddiqi S. Ghaffar A, Sadiq II. (Eds.). Strengthening of TB.
10.Liefooghe R, Moran MB, habib S, De Muynck A. Treatment adherence of tuberculosis patients in Bethania Hospital, Sialkot. J. C. P. S. P. 1997; 7: 140-4.
11.Sloan JP. Sloan MC. An assessment of’ default and non-compliance in tuberculosis control in Pakistan. Trans. R. Soc. Trop. Med. Hyg., 1981; 75: 717-18.
12.Liefooghe R. The human dimension in TB control: myth or reality? In: Meulemans H. (Ed) Tuberculosis in Pakistan: The forgotten plague. Acco, Leuyen, Cahier Faculty of Political and social sciences, 2000, 19.pp. 41-53.
13.Liefooghe R, Michiels N, Habib S. et al. Perception and social consequences of tuberculosis: a focus group study of tuberculosis patients in Sialkot. Pakistan. Soc. Sci. Med. 1995: 4 1: 685-92.
14.Directorate of Tuberculosis Control. National Guidlines for Tuberculosis Control in Pakistan, Islamabad, Federal Ministry of Health. 1995.
15.Asamoa K. Social conselling and tuberculosis treatment adherence at Bethania Hospital S ialkot, Pakistan. Disseration, Postgraduate Masters of science Course Community Health Management in Developing Countries”. Institute of Tropical Hygiene and public Health. University of Heidelberg, 1998.
16.Liefooghe R. Suetens C, Meulemans II, et al. A randomised trial of the impact of counselling on treatment adherence of Tuberculosis Patients in Sialkot, Pakistan. Int. J. Tubercle Lung Dis.. 1999; 3: 1073-1080.
17.De Muynck A, Liefooghc R. Moran MB. Is the use of survival analysis relevant in the study of compliance patterns in tuberculosis?~Abstract]. Tubercle Lung Dis., 1996; 77: 76.
18.Hanza A. The two biraderis: kinship in rural West Punjab. In: Madan TN. Manohar (Eds). NcwDelhi. Mulim communities of SouthAsia, 1995. pp. 1-62.
19.Sumartojo, F. When tuberculosis treatment fails. A social behavioral account of patient adherence. Am. Rev. Respir. Dis., 1993; 147, 1311-1320.
20.Ruhcl AJ. Garro LC. Social and Cultural factors in the successful control of tuberculosis. Public Health Rep. 1992; 107, 626-636.
21.Seetha MA, Srikantaraniu N, Aneja KS et al. influence of motivation of patients and their family members on the drug collection by patients. Indian J. Tubercle., 1981; 28: 182-190.
22.Uplekar M and Rangan S. People’s awareness and patients perceptions. In: Tackling TB. The search for solutions. Bombay. The foundation for research and community health. 1996, pp. 9-31.
23.Liam KC, l.im KH, Wong CMM et al. Attitudes and knowledge of newly diagnosed tuberculosis patients regarding the disease, and factors affecting treatment compliance. tnt. J. Tubercie Lung Dis., 1999; 3: 300-9.
24.Barhoorn F, Adriaanse H. In search of factors responsible for noncompliance among Tuberculosis patients in Wardha Distric. India. Soc. Sci. Med., 1992; 34, 29 1-306.
25.SPDC tern. Social development in Pakistan. Annual review 1998. Karachi. Social Policy and Development Centre, 1998.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: