
J. Usman ( Department of Family Medicine, Ziauddin Medical University, Karachi. )
November 2002, Volume 52, Issue 11
Family Medicine Corner
Introduction
Obesity is rapidly becoming a major public health problem. The health implications of obesity are so serious that it has been designated a leading cause of preventable death (second only to smoking) in the US1. WHO in 1997 declared obesity as posing serious threat to public health due to increased risks of related co-morbidity including hypertension, coronary artery disease and type 2 diabetes mellitus2.
It is not a difficult condition to recognize and can be best treated in the context of the patient’s family and environment.
Definition
Obesity can be defined as an excessive body fat content. Body Mass Index (BMI: the body weight in kilograms divided by the square of the height in meters).
Measurements of waist circumference or the ratio of the waist to the hip circumference provide information about fat distribution, which is an important factor, in the co- morbidity associated with obesity, as greater risks are associated with an abdominal distribution of fat (a large waist circumference,’apple shaped’ than with a peripheral distribution pear- shaped4.
Current evidence suggest that abdominal obesity, previously described by Jean Vague, a French physician in mid forties as “ android obesity” carries a major risk for cardiovascular complications as compared to accumulation of fat in the gluteo-femoral region commonly found in premenopausal women described by him as “gynoid obesity”5.
Studies using Imaging techniques such as magnetic resonance imaging (MRI) and computed tomography (CT) that can distinguish between intra-abdominal or visceral fat depot from subcutaneous abdominal fat, reveal waist circumference as a predictable anthropometrics marker of the amount of visceral fat5..
Etiology
The cause of obesity is multi-factorial, with a strong influence by modifiable and preventable environmental factors, however, there is no doubt that obesity is also influenced by genetics6. The pattern of inheritance is polygenic, and with the identification of the leptin genes, many other single genes have been investigated, and studies are underway to scan the loci associated with obesity.
Obesity is commonly associated with the development of various diseases (Table).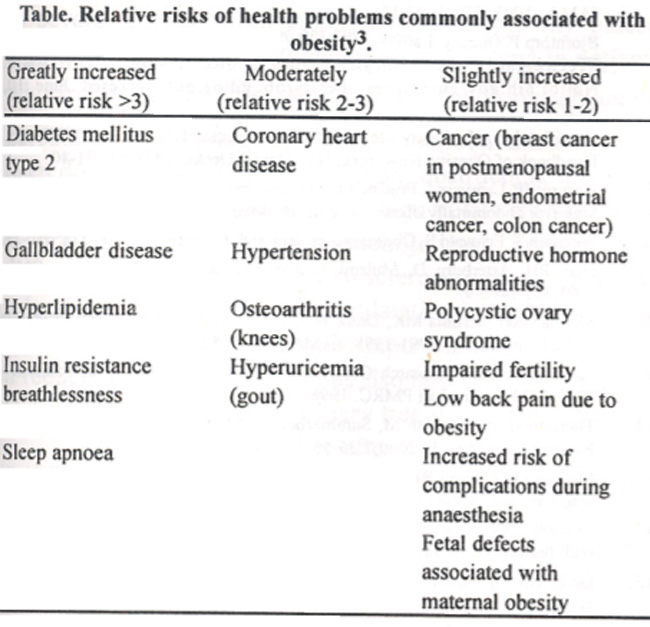
Prevalence
Obesity has increased steadily in certain countries since 1900. In the UK in 1994, it was estimated that 13% of men and 16% of women were obese7. The prevalence of obesity in the US has increased from 12.0% in 1991 to 17.9% in 19988.
In Pakistan levels of obesity tend to increase with age. It has been found to be more common among females, 40 percent of urban women 45-64 years of age are obese. Among the 25-44 years age group 9 percent of rural males are obese as compared to 22 percent urban males, whereas 14 percent of rural females of the same age group were obese as compared to 37 percent of urban females9. The prevalence of obesity for children 5-14 years is not documented. Hypertension and Diabetes Mellitus are highly prevalent among obese and overweight Pakistanis. In Pakistan circulatory diseases cause over 100,000 deaths a year, 12 percent of all deaths annually9.
Evaluation
In clinical practice obesity can be determined by using two methods, one is to estimate the ideal body weight by using the BMI table, the other more accurate is the measurement of adiposity by measuring skin fold thickness through the use of calipers. By testing the skin fold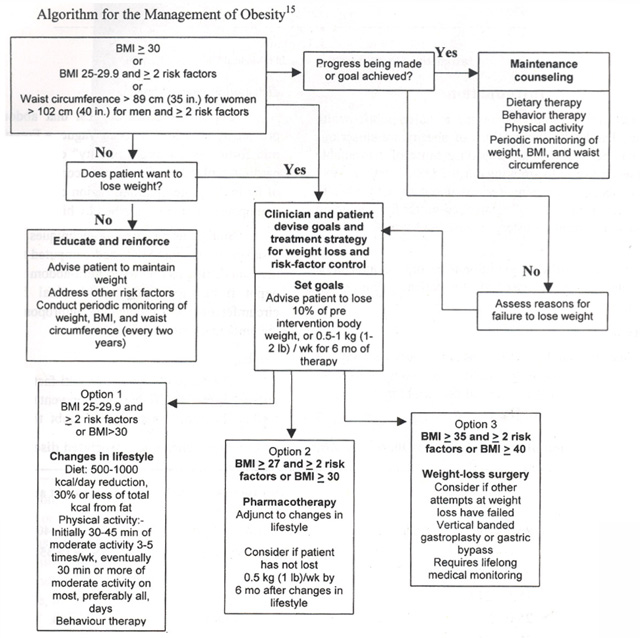
thickness at predetermined anatomical points, the examiner can estimate the ratio of adipose tissue to lean body mass. Skin fold thickness is very helpful in long-term counseling in weight reduction because it directly measures the adipose tissue.
Obesity in the abdominal areas carries the greatest risk. In men, the risk of waist/hip ratio (waist circumference divided by hip circumference) is a risk factor for ischemic heart disease, diabetes, stroke and death. In men, the risk increase significantly when the waist/hip ratio rises above 1:1, and in women when it is above 0.8:1. This is independent of total body fat mass5.
Screening
A close relation between accumulation of visceral adipose tissue and plasma insulin and apolipoprotein B has been reported6. A ‘triad’ of atherogenic risk markers have been identified. Fasting hyperinsulinemia, increased apolipoprotein B concentration, and an increased low density lipoprotein particles (abnormalities found in viscerally obese men, even in the absence of type 2 diabetes mellitus), are important factors.
Accumulation of visceral fat can be estimated by anthropometrics indices and waist circumference is a useful measurement not only to predict accumulation but also to monitor its change over time.
Simple screening variables, such as waist circumference and fasting triglyceride concentration can identify high risk obese men who would be carriers of the atherogenic triad. This has been defined as “Hypertriglyceridemic waist” a new clinical phenotype defining high risk form of obesity. A cut off value of waist measurement> 90 cm and triglyceride concentration> 2 mmol / L characterizes this phenotype5.
Approach to management
Obesity should be considered a disease. A family physician must realize that several steps need to be taken to help obese patients lose weight. Counseling and convincing in losing weight is the hallmark of any strategy adopted. Obese patients needs support and positive reinforcement throughout the weight loss process.
Health education about the medical consequences of obesity and nutritional information is important. The family physician also needs to work with the individual in setting goals and sub goals. Including family members in the treatment plan can work as a good source of positive reinforcement. Family physicians need to be aware of various approaches to management.
The approaches towards management include non-pharmacological as well as pharmacological. Systematic reviews and Randomized Controlled Trials (RCT) have found that a combination of advice on diet and exercise, supported by behavioral therapy, is more effective in achieving weight loss than either diet or exercise alone10. A low energy, low fat diet is the most effective lifestyle intervention for weight loss. One systematic review and five randomized controlled trials have found that most strategies that involve personal contact with a therapist, family support, multiple intervention, or are weight focused appear to be most effective11.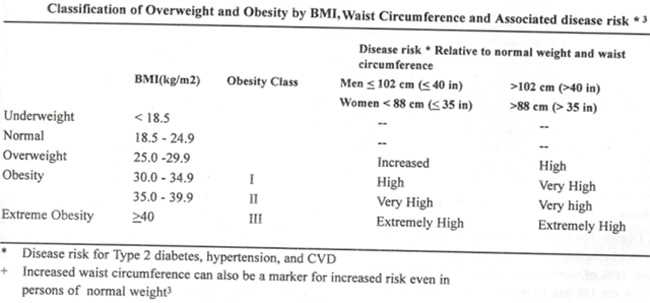
Pharmacological treatments involve a number of drugs that includes centrally acting drugs such as Phenylpropanolamine, Phentermine, Mazindol, Diethylproprion, Fluoxetine, Dexfenfluramine, Fenfluramine, Fenfluramine plus phentermine and the newer drugs Orlistat and Sibutramine.
Phenylpropanolamine, phentermine, mazindol and diethylproprion result in modest weight loss in people more than 15% overweight. Serious adverse effects such as intracranial hemorrhage, acute psychotic reactions, hypertensive episodes and seizures preclude their prescription. Dexfenfluramine and combination of fenfluramine with phentermine have been associated with valvular heart disease and pulmonary hypertension12. Two randomized controlled trials found limited and conflicting evidence comparing fluoxetine with placebo13.
Among the newer drugs Orlistat (Xenical) that binds to gastrointestinal lipases in the lumen of the gut, prevent hydrolysis of dietary fat (triglycerides) into absorbable free
fatty acids and monoacelyglycerols, when combined with a low calorie diet has shown to increase the weight loss in adults with obesity. Weight gain following discontinuation has not been reported. Oily spotting from the rectum and flatulence has been reported in 22-27% of people taking orlistat. Limited evidence from six RCTs suggests that sibutramine (Reductil) an inhibitor of both norepinephrine and serotinin reuptake and weak inhibitor of dopamine reuptake, can increase weight loss in healthy adults with BMI between 27-40 kg/m214.
Selected patients with a body mass index of at least 40 or less along with obesity related medical conditions can benefit from bariatric surgical treatments, such as gastric bypass15.
Many approaches can be used in combination, and long-term lifestyle change should be the ultimate goal of management. With the identification of high risks associated with obesity, family physicians should treat by focusing on therapeutic targets.
References
1.McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA., 1993; 270: 2207-12.
2.Bjorntorp P. Obesity. Lancet, 1997;350 997-1000.
3.Clinical guidelines on the identification, evaluation and treatment of overweight and obesity in adults. http: // www.Nhlibi.nih.gov/guidelines/obesity/ob_gdlns.pdf (accesed June 10,2002),
4.Bray GA, Bouchard C, James WPT. Definitions and proposed current classification of obesity. In: Bray GA, Bouchard C, James WPT, eds. Handbook of Obesity. New York, NY: Marcel Decke, 1998, pp. 31-40.
5.Despres JP, Lemieux I, Prud’homme D. Treatment of obesity: need to focus on high risk abdominally obese patients. Br. Med .J., 2001; 322: 716-20.
6.Sorensen 1, Echwald S. Obesity genes, editorial. Br. Med. J., 2001; 322: 630-31.
7.Noel PH, Arterbum D, Mulrow C. Obesity. In: Clinical evidence. BMJ., 2001;322:1406-9.
8.Mokdad AH, Serdula MK, Dietz WE, et al. The spread of obesity epidemic in the United States 1991-1998. JAMA., 1999 282:1519-22.
9.Pakistan Medical Research Council: National Health Survey of Pakistan - 1990-1994., Islamabad PMRC.,1998.
10.Thorogood M, Hillsdon M, Summerbell C. Changing behavior. In: Clinical Evidence. Br. Med. J., 2000;7:36-56.
11.McGuire MT, Wing RR, Kien ML, et al. Behavioral strategies of individuals who have maintained long-term weight losses. Obes. Res., 1 999;7:334-41.
12.Connolly HM, Crary JL, Mcgoon M, et al. Valvular Heart disease associated with fenfluramine-phentermine. N. EngI. J. Med., 1997;337: 581-88.
13.Goldstein DJ. Ranipey AN Jr, Enas CG, et al. Fluoxetine: a randomized clinical trial in the treatment of obesity. Int. J. Obes., 1994;18 129-35.
14.Yanovski SZ, Yanovski JA. Obesity. New EngI. J. Mcd,. 2002;346:591-602.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: