
A. Abbas ( Department of Ophthalmology, The Aga Khan University, Karachi. )
B. Khan ( Department of Ophthalmology, The Aga Khan University, Karachi. )
A.H. Feroze ( 37th and 0 Streets, NW, Washington, DC 20057, USA, Boulevard, Brooklyn, NY 11212, USA. )
G.F. Hyman ( Brookdale University Hospital Medical Centre, Boulevard, Brooklyn, NY 11212, USA. )
October 2002, Volume 52, Issue 10
Original Article
Abstract
Objective: Thalidomide is a potent inhibitor of angiogenesis. We evaluated the effects of Thalidomide on comeal angiogenesis and on tissue survival of grafts in rabbit eyes with pre-existing neovascularization secondary to alkali bum.
Methods: Sixteen rabbits received alkali bums to one cornea. One month post-injury, assessments of comeal neovascularization were performed followed by corneal transplantation. Four rabbits received oral Thalidomide and ten got placebo (powdered sugar) for thirty days. Total comeal neovascularization (NV), clock hours (CH) involved in (NV), longest (NV) pedicle length (NVP) and the duration of time required for NV to develop were assessed.
Results: Thalidomide significantly decreased the total neovascularization (p<0.0072), the number of(CH) involved (p<0.0002) and the longest (NVP) length (p<0.0001). There was also a significant delay in the earliest development of NV in the test group (p<0.0064). The test group retained comeal clarity significantly longer than the control group (p< 0.0008).
Conclusion: Thalidomide is an effective inhibitor of corneal angiogenesis and prolongs graft survival as measured by graft clarity in donor corneas in eyes with previous neovascularization secondary to alkali injury.
Clinical Relevance: Thalidomide may be used as a modulator of corneal angiogenesis to prolong graft survival in eyes with pre-existing corneal neovascularization (JPMA 52:476;2002).
Introduction
The first successfully transplanted solid tissue was the cornea1. The observation that corneas were less frequently rejected compared to other tissues lead to the belief that the cornea enjoyed “Immunologic Privilege”. This view is substantiated by the observation that vascularized and pre-sensitized recipients reject comeal grafts more frequently than non-vascularized recipients2,3.
Cornea! graft rejection in uncomplicated cases occurs in about 3-35 % of the times. The incidence in high-risk cases with inflammation and neovascularization increases to 40-65 %2,4. We were interested in reducing this neovascularization so as to improve the chances of graft survival.
Thalidomide was developed in the 1950’s by Chemie-Grunenthal as a sedative and was so nontoxic in rodents that an LD 50 could not be established. In 1961.
McBride5 and Lenz6 described an association between Thalidomide use in pregnant women and limb defects in their babies. These teratogenic effects were reproduced in rabbits at 100-300 mg/kg/day7,8. It has been postulated that the limb defects occurred as a result of the direct inhibitory effect of Thalidomide on angiogenesis in the developing limb bud9,10. With this knowledge we chose rabbits for our study. Thalidomide has been re-introduced into the US market for erythema nodosum leprosum and the skin manifestations of lupus erythematosus.
In the past decade, there has been renewed interest in the antiangiogenic activity of this drug, especially in Cancer research and Transplantation12,18.
Owing to its potent anti-angiogenic properties, Thalidomide would prevent or significantly retard the growth of vessels into the donor cornea reducing the exposure of foreign tissue to the host defense mechanisms, hence reducing the chances of rejection. D’Amato et al studied the effects of oral Thalidomide on comeal angiogenesis, which they had experimentally produced in rabbit corneas using basic fibroblast growth factor19. Their study demonstrated a significant inhibition of corneal neovascularization in the Thalidomide group (200mg/kg/day). This antiangiogenic effect was observed after only two doses and was comparable to the drug’s teratogenic properties. Later, Kruse et a! showed the same effect when they induced comeal neovascularization with vascular endothelial growth factor (VEGF)20.
This study evaluates the effects of Thalidomide in preventing neovascularization in corneal graft donor buttons in rabbit eyes that have pre-existing neovascu!arization secondary to alkali burns.
Materials and Method
Corneal neovascularization was induced in the left eye of sixteen male New Zealand white rabbits, average weight 2.77 Kg. All animals were handled in accordance with the National Institute of Health guidelines on the care
C/12 x 3.1416 - (r - L)2] where, r = radius of the cornea, C = number of clock hours of limbus involved with neovascularization and L = Maximum vascular pedicle length from host-graft interface onto donor cornea.
L = length of the longest vascular pedicle from the limbus onto anterior cornea.
The rabbits were then assigned randomly and in a double blinded manner to a test and a control group. The test group had four and the control group, twelve rabbits. Penetrating keratoplasty was performed on the vascularized left eye of fifteen rabbits, using an 8 mm corneal graft obtained from a healthy rabbit, sutured into a 7.5 mm host interface, using sixteen to eighteen 10-0 nylon interrupted sutures. Post-operatively, Tobramycin + Dexamethasone ointment was instilled and the eye was patched overnight. Starting on post-operative day one, the four test rabbits were fed in a blinded fashion, 200 mg/Kg/day of Thalidomide for 30 days. The control group received placebo in the form of powdered sugar. In addition, the eyes received Pred-forte 1% eye drops QID for 30 days and Ciprofloxacil HCL eye drops QID tapered off over two weeks. Daily examinations were performed to assess the development of infectious keratitis, corneal rejection, maintenance of cornea! clarity (Table 1) and the development of corneal graft neovascularization. On day 30, an assessment of corneal neovascularization was performed with the above mentioned equation, where r = Radius of the donor cornea, (4.0 mm).
C = Number of clock hours of host-graft interface involved with neovascularization,
Following this, the rabbits were euthanized in accordance with the aforementioned guidelines. The results were assimilated and the study unmasked. Data was entered and analyzed using the computer software SPSS version 10.0 for Windows. Independent samples’ t-test was used to assess the efficacy of Thalidomide in preventing neovascularization of the comeal graft.
Results
Sixteen male New Zealand white rabbits, average weight 2.77 Kg suffered the initial alkali injury to their left corneas and underwent the pre-operative recovery and neovascularization phase of four weeks. During this preoperative (pre-thalidomide) recovery period, the control and the test groups did not exhibit any clinically significant differences in the time of earliest detection of corneal neovascularization, the number of clock hours (C) involved in the neo-vascular response, longest neo-vascular pedicle length (L) from limbus onto anterior cornea, and the amount of total cornea! surface area involved in neovascularization, (Table 1).
At the end of this period one rabbit was found to have a large central descemetocele and was removed from the study, as the cornea was not transplantable. Fifteen rabbits thus underwent successful penetrating keratoplasty. During the post-operative period, one rabbit developed severe keratitis and endophthalmitis and was removed from the study. Both these rabbits belonged to the control group. Fourteen rabbits completed the study (n14), (Table 1).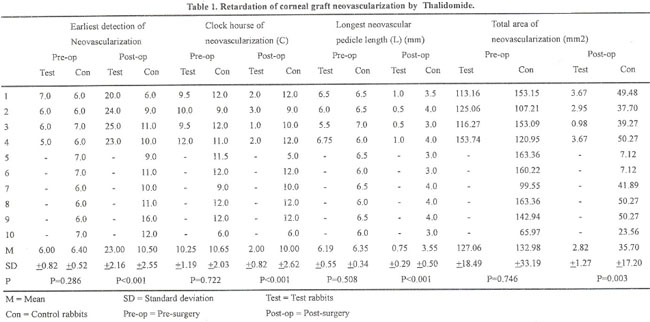 In the control group, earliest evidence of donor tissue neovascularization was detected significantly earlier than the test group. The test group had significantly less clock hours (C) of donor corneal circumference involved in neovascularization than the control group. The longest neovascular pedcle length (L) was significantly shorter in the test group than in the control group. The total area of donor cornea involved in neovascularization in the test group at the end of the study was significantly less than the control group (Figures 1 and 2).
In the control group, earliest evidence of donor tissue neovascularization was detected significantly earlier than the test group. The test group had significantly less clock hours (C) of donor corneal circumference involved in neovascularization than the control group. The longest neovascular pedcle length (L) was significantly shorter in the test group than in the control group. The total area of donor cornea involved in neovascularization in the test group at the end of the study was significantly less than the control group (Figures 1 and 2).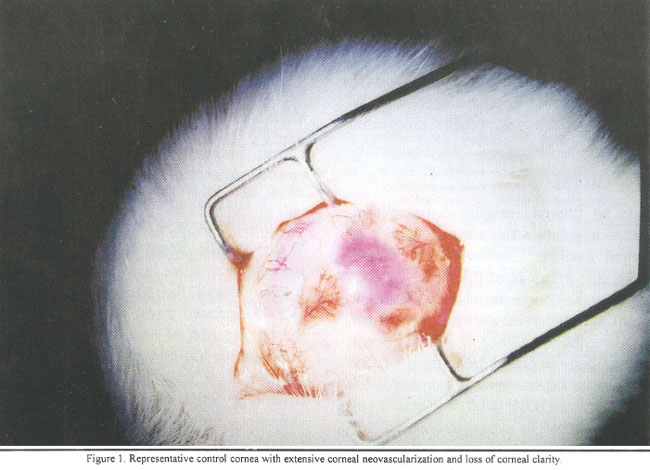
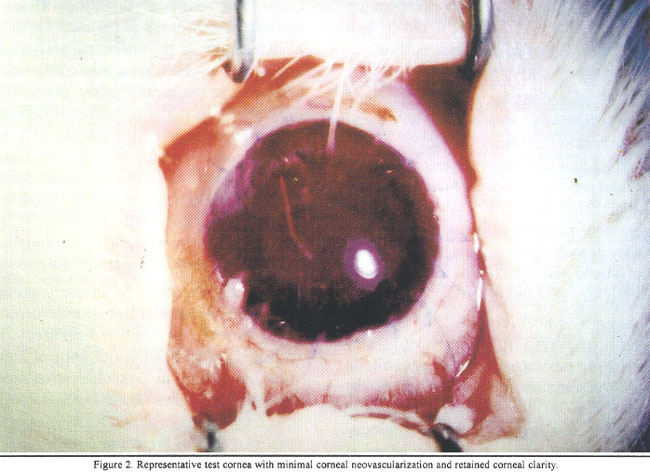
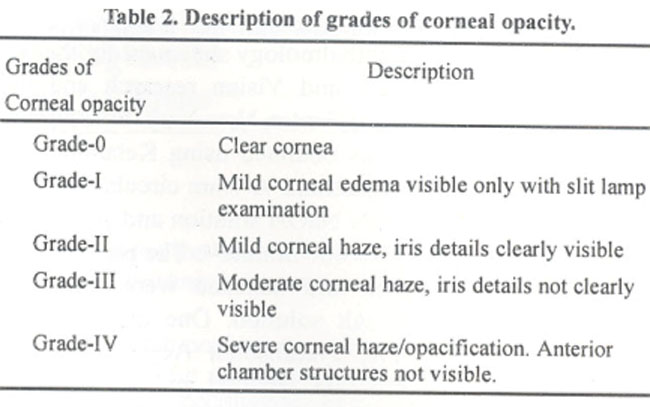
Table 2 describes the different grades of corneal opacity.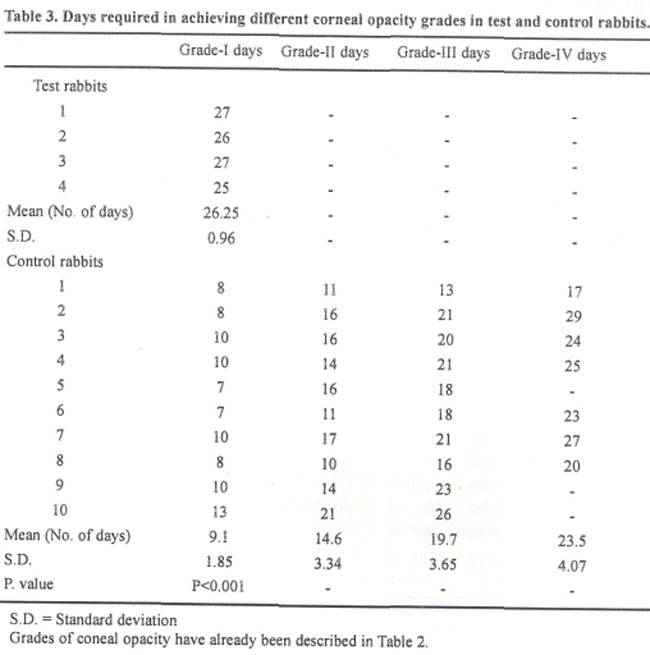 Table 3 demonstrates that all the rabbits reached grade I comeal opacification. However, the control group required significantly fewer days to reach this level of corneal opacification compared to the test group. All of the rabbits in the control group reached grade II and grade III. Seven often rabbits in the control group developed grade IV opacification while none of the test rabbits progressed beyond grade I (Figures 1 and 2).
Table 3 demonstrates that all the rabbits reached grade I comeal opacification. However, the control group required significantly fewer days to reach this level of corneal opacification compared to the test group. All of the rabbits in the control group reached grade II and grade III. Seven often rabbits in the control group developed grade IV opacification while none of the test rabbits progressed beyond grade I (Figures 1 and 2).
Discussion
The cornea is an immune privileged tissue that, when grafted orthotopically forms the anterior surface of the immune privileged anterior chamber22, The factors responsible for this include presence of the blood-aqueous barrier, the avascularity of the cornea, the absence of classic antigen-presenting cells (APCs) in the central cornea, inhibitory factors in the aqueous humor, the phenomenon known as anterior chamber-associated immune deviation (ACAID) and the intraocular expression of Fas ligand. Loss of ocular immune privilege can occur with a breach in any or all of these mechanisms23,24. The eyes are rendered high risk, at least in part, by virtue ofcomeal neovascularization failing to provide immune privilege for orthotopic corneal allografts. Neovascularization creates graft beds in which recipient antigen-presenting cells infiltrate the graft and carry antigenic information by lymphatics to draining lymph nodes. In this manner, ACAID is avoided, and potentially allodestructive Delayed Hypersensitivity is promoted25.
The cornea plays an active role in ocular immune privilege and ACAID by creating a local immunosuppressive microenvironment, providing neural afferent stimuli that affect immunosuppressive properties of Iris and Ciliary body, and preventing neovascularization and infiltration with Langerhan’s cells26. Corneal endothelial cells inhibit antigen and mitogen-activated lymphocyte proliferation27-29. Neuropeptides play also an important role in ocular immune privilege and creation of an intraocular immunosuppressive microenvironment30-31.
The corneal graft contributes to its immune privileged status in three ways: (a) absence of donor-derived, antigen-presenting passenger Langerhan’s cells in the comeal graft; (b) expression of Fas ligand on the epithelium and endothelium of the corneal allograft and (c) capacity of the corneal allograft to induce immune deviation of the systemic immune response32. Corneal allografts induce cytotoxic T cell but not delayed hypersensitivity responses33. Apoptosis of infiltrating cells on the corneal endothelium resulting from Fas-FasL interaction plays an important role in the high success rate of comeal transplantation. Yamagami et al and Stuart et al showed that the rejection rate in the FasL - group (89%) is significantly higher than in the FasL+ control group (47%)34-36
The donor-derived Langerhan’s cells act as Antigen Presenting Cells (APCs) in the induction of delayed type hypersensitivity responsiveness to allergenic tissue37, The presence and persistence of Langerhan’s cells in diseased corneas may account for, at least in part, a breakdown of comeal immune privilege with a higher rate of rejection episodes after comeal transplantation38.
Thalidomide, after hydrolysis to active metabolites, specifically binds to GC promoters and inhibits expression of ß2 and (33 integrin subunits by the leukocytes39-41. pzintegrins mediate leukocyte adhesion to the endothelium. It also blocks the Vascular Endothelial Growth Factor (VEGF)-induced down regulation of caveolin-1, vital for the propagation of endothelial cells20,42,43. In rat models, Thalidomide has an immunosuppressive effect pronounced enough to replace corticosteroids after lung transplantation13. It also upregulates the IL-4 and IL-5 expression, favoring TH2-type response over TH 1-type response. In Cancer Research, it has also been shown to decrease Tumor Necrosis Factor - alpha (TNF-ct) production by human monocytes, and raise Reactive Oxygen Species (ROS) levels44.
The results of this study clearly demonstrate the extreme effectiveness of thalidomide in decreasing the rate of development of donor corneal neovascularization as manifested by later detection of donor neovascularization compared to the control group. Also, Thalidomide reduces the severity of the total neovascular response as shown by decreased number of clock hours (C) involved, decreased neo-vascular pedicle length (L) from the host-donor interface onto donor cornea and decreased total donor comeal surface area involved in the pannus. The study shows increased graft survival, with the test group maintaining corneal clarity for a longer period of time as compared to the control group.
Oral Thalidomide, in conjunction with the present-day therapy for alkali bums, exceptionally retards the development of and decreases the severity of neovascularization of donor comeal buttons in rabbit eyes with pre-existing neovascularization secondary to previous alkali corneal burns. There is also a marked increase in the longevity of functional graft tissue as evidenced by retained comeal clarity of the donor tissue.
There might be some concern about the reproducibility of the induced corneal angiogenesis by our injury model. However, this model has successfully been used in the past and our own pre-operative findings (Table 2) indicate reproducible and consistent neovascularization induction. Thalidomide has previously been shown to be effective in retarding neovascularization in both the FGF-ßand VEGF models of induced comeal angiogenesis. We decided to assess the same in an alkali bum model as it reflects real life scenarios experienced by clinicians. Even though our sample size is small, the results are credible enough to be reported. Further studies need to be performed in order to assess the benefits of continued use of Thalidomide as well as the ideal dosage.
If Thalidomide is ever considered for use as a corneal anti-angiogenic agent, its use will have to be restricted to male patients and to women who are willing to perform at least two forms of contraception, chemical and barrier, in addition to understanding the necessity of abortion if conception were indeed to occur during Thalidomide use.
Acknowledgements
We thank Syed Iqbal Azam, Senior Instructor, CHS Department, Aga Khan University, Karachi and Sajjad Akhtar, M.D. for their help in performing the statistical analysis for this article. We also thank Dr. Peter Andrulis of Andrulis Pharmaceuticals for providing the thalidomide for this study.
References
1.Silverstein AM, Khodadoust AA. Transplantation immunology in the cornea. In: Jones BR (ed). Corneal graft failure - Ciba foundation Symposium. Amsterdam: Elsevier, 1973, p. 105.
2.Chandler JW, Kaufman HE, Graft reactions after keratoplasty for keratoconnus. Am.J. Ophthalmol., I 974;77 :543.
3.Stark WJ, Opelz G, Newsome D, et al. Sensitization to human lymphocyte antigens by corneal transplantation. Invest. Ophthalmol,1973;12:639.
4.Khodadoust AA, Silverstein AM. Transplantation and rejection of individual layers of the cornea.Invst. Ophthalmol., 1969;8:169.
5.McBride WG. Thalidomide and congenital anomalies. Lancet, 1961;ii:1358.
6.Lenz W. Thalidomide and congenital anomalies. Lancet, 1962;i:45.
7.Helm F. ierexperimentelle untersuchungen and dysmeliesyndrom] Studies in experiment animals and dysmelia syndrome. Arzneiimforschung, 1966;l6: 1232.
8.Sterz H, Notduft H, Lexa P, et al. Teratologicstudies on the Himalayan rabbit: new aspects of thalidomide-induced teratogenesis. Arch. Toxicol., 1987;60:376-81.
9.Stephens TD, Fillmore BJ.Hypothesis: thalidomide embryopathy-proposed mechanism of action. Teratology, 2000;61 :189-95.
10.Sauer H, Gunther 3, Hescheler J, et al. Thalidomide inhibits angiogenesis in embryoid bodies by the generation of hydroxyl radicals. Am.J.Pathol.,2000;1 56:151-58.
11.Joussen AM, Germann 1, Kirchhof B. Effect of thalidomide and structurally related compounds on conical angiogenesis is comparable to their teratological potency. Graefes. Arch. Clin. Exp. Ophthalmot., 1999;237:952-61.
12.Rajkumar SV, Witzig TE. A review of angiogenesis and antiangiogenic therapy with thalidomide in multiple myeloma. Cancer, Treat. Rev., 2000;26:351-62.
13.Jakkula M, LeCras TD, Gebb S, et al. Inhibition of angiogenesis decreases alveolarization in the developing rat lung. Am.J.Physiol. Lung Cell Mol. Physiol., 2000;279:L600-7
14.Anonymous. A cautious comeback for thalidomide. Harv. Health Left., 1 998;23:4-5.
15.Marriott JB, Muller G, Dalgleish AG. Thalidomide as an emerging immunotherapeutic agent. Immunol. Today, 1 999;20:538-40.
16.Miller MT, Stromland K. Teratogen update: thalidomide: a revew with a focus on ocular findings and new potential uses. Teratology, 1999;60:306-21.
17.Ziegler J. Angiogenesis research enjoy growth spurt in the 1990s. J.Natl. Cancer Inst., 1996;88:786-88.
18.Verheul HM, Panigrahy D, Yuan J, et al. Combination oral antiangiogenic therapy with thalidomide and sulindac inhibits tumor growth in rabbits. Br.J.Cancer, 1999;79:1 14-18.
19.DAmato Ri, Loughman MS, Flynn E, et al. Thalidomide is an inhibitor of angiogenesis. Proc.NatI.Acad.Sci.,l 994;91 :4082-85.
20.Kruse FE, Joussen AM, Rohrschneider K, et al. Thalidomide inhibits comealangiogenesis induced by vascular endothelial growth factor. Graefes. Arch. Clin. Exp. Ophthalmol., 1998;236:461-66.
21.Hayashi K, Ishibashi T. In vivo observations on experimental conical neovascularization with a newly developed macroscope. Graefes. Arch. Clin. Exp.Ophthalmol., 1991 ;229:473-79.
22.Tanaka K, Yamada J, Joyce N, et al. Immunobiology of xenogeneic cornea grafts in mouse eyes. I. Fate of xenogencic cornea tissue grafts implanted in anterior chamber of mouse eyes. Transplantation, 2000;69:6 10-16.
23.Rocha G, deschenes J, Rrowsey JJ. The immunology of conical graft rejection. Crit. Rev. Immunol., 1998;18:305-25.
24.Dana Mr, Streilcin JW. Loss and restoration of immune privilege in eyes with conical neovascularization. Invest. Ophthalmol. Vis. Sc, 1996;37:2485-94.
25.Sano Y, Ksander BR, Streilein JW. Fate of orthotopic conical allografts in eyes that cannot support anterior chamber-associated immune deviation induction. Invest. Ophthalmol. Vis. Sci.,1995;36:2176-85.
26.Streilein JW, Bradley D, Sano Y, et al Immunosuppressive properties of tissues obtained from eyes with experimentally manipulated comeas. Invest. Ophthalmol. Vis. Sci., I 996;37:41 3-24.
27.Hon J, Joyce NC, Streilein 3W. Immune privilege and immunogenicity reside among different layers of the mouse cornea. Invest.Ophthalmol.Vis.Sci., 2000;4l :3032-42.
28.Hon J, Joyce N, Streilein JW. Epithelium-deficient conical allografis display immune privilege beneath the kidney capsule. Invest. Ophthalmol. Vis. Sci., 2000;41:443-52.
29.Mi P, Gregerson DS, Kawashima H. Local regulation of immune responses: conical endothelial cells alter T-cell activation and cytokine production. Cytokine, 2000;12:253-64.
30.Taylor AW, Streilein JW, Cousins SW. Immunoreactive vasoactive intestinal peptide contributes to the immunosuppressive activity of normal aqueous humor. J. Immunol., 1994; 153:1080-6.
31.Taylor AW. Neuroimmunomodulation in immune privilege: role of neuropeptides in ocular immunosuppression. Neuroimmunomodulation, 1996;3:195-204.
32.Niederkom JY The immune privilege of conical allografls. Transplantation, 1999;67: 1503-8.
33.Peeler 3, Niederkom J, Matoba A. Conical allografts induce cytotoxic T cell but not delayed hypersensitivity responses in mice. Invest. Ophihalmol. Via. Sci., 1985;26:1516-23.
34.Ross J, Callanan D, Kunz H, et al Evidence that the fate of class TI-disparate conical grafts is determined by the timing of class II expression. Transplantation, 1991 ;5 1:532-36.
35.Yamagami S. Kawashima H, Tsuru T, et al Role of Fas-Fas ligand interactions in the immunorejection of allogeneic mouse conical transplants. Transplantation, 1 997;64: 1107-11.
36.Stuart PM, Griffith TS, Usui N, et al CD95 ligand (FasL)-induced apoptosis is necessary for conical allograft survival. J.Clin.Invest., l997;99:396-402.
37.Peeler JS, Niederkom JY. Antigen presentation by Langerhan’s cells in vivo: donor-derived Ia+ Langerhan’s cells are required for induction of delayed-type hypersensitivity but not for cytotoxic T lymphocyte responses to alloantigens. J. Immunol.,1 986; 136:4362-71.
38.Philipp W, Gottinger W. Zur Haufigkeit und Funktion von Langerhans-Zellen bei verschiedenen Homhauterkrankungen.
40.Kenyon BM, Browne F, D’Amato RJ. Effects of thalidomide and related metabolites in a mouse comeal model of neovascularization. Exp. Eye. Res., 1997;64:97 1-78.
41.McCarty MF. Thalidomide may impede cell migration in primates by down-regulating integrin beta-chains: potential therapeutic utility in solid malignancies, proliferative retinopathy, inflammatory disorders, neointimal hyprplasia and osteoporosis. Med.Hypotheses, 1997;49:123-31.
42.Liekens S. De Clercq E, Neyts J. Angogenesis: regulators and clinical applications. Biochem. Pharmacol., 2001 ;61 :253-70.
43.Liu J, Razani B, Tang S, et al. Angiogenesis activators and inhibitors differentially regulate caveolin-1 expression and caveolae formation in vascular endothelial cells. Angiogenesis inhibitors block vascular endothelial growth factor-induced down-regulation of caveolin-1. J. Biol. Chem., 1999;274:781-5.
44. Kotoh T, Dhar DK, Masunaga R, et al. Antiangiogenic therapy of human oesophageal cancers with thalidomide in nude mice. Surgery, 1999;125:536-44.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: