
I. Siddiqui ( Departments of Pathology, The Aga Khan University Hospital, Karachi. )
H. S. Bhally ( Departments of Medicine, The Aga Khan University Hospital, Karachi. )
Q. Niaz ( Departments of Medicine, The Aga Khan University Hospital, Karachi. )
I. A. Burney ( Departments of Medicine, The Aga Khan University Hospital, Karachi. )
August 2002, Volume 52, Issue 8
Original Article
Abstract
Objective: To delineate the demographics and predictors of early mortality associated with tumor-induced hypercalcemia (TIH) amongst cancer patients in Pakistan.
Setting: A tertiary care hospital in Pakistan.
Patients and Methods: Retrospective analysis of patients with cancers, presenting with TIH and admitted to the hospital between January1988 and December 1997, was carried out.
Results: Eighty-four patients (56 males and 28 females) were diagnosed to have TIH. The mean age at the time of presentation was 55±14 years. Twenty-five percent of the patients each had multiple myeloma and hepatocellular carcinoma whereas 20% of the patients had underlying breast cancer. Other malignancies included lung cancer, gall bladder cancer and colorectal carcinomas.
Univariate analysis revealed male sex (p <0.04), underlying diagnosis other than multiple myeloma (p <0.025) and a high TLC (p <0.05) at presentation, as predictors of an early mortality.
Conclusion: Multiple myeloma, hepatoma and breast carcinoma were common cancers causing TIH. One-third patients died within first few days. Male sex, a high white cell count and an underlying diagnosis other than multiple myeloma predicted early mortality (JPMA 52:361; 2002).
Introduction
Tumor-induced hypercalcemia (TIH) is the second most common paraneoplastic syndrome following cancer associated cachexia syndrome (CACS)1,2. The incidence of TIH amongst advanced malignancies is reported to be 5-20%3. TIH is essentially due to a marked increase in osteoclast-mediated bone resorption. Parathyroid-hormonerelated protein (PTH-rp) also plays an essential role in causing TIH4.
Generally, the underlying disease is incurable however, treatment of TIH may improve quality of life5. Symptoms related to the Central Nervous System (CNS) and to intravascular volume depletion can be controlled with effective anti-hypercalcemia therapy in more than 70% of cases. Serum calcium levels also decrease to within normal limits in about 40-80% of cases. TIH occurs most commonly secondary to cancers of breast, lungs, prostate and myeloma6. The different patterns of cancers and late presentation in our country may mean that the outcome of patients presenting with hypercalcemia in this part of the world may be different to what has been reported in the literature7,8.
The objective of this study was to delineate the demographics and predictors of early mortality associated with tumor-induced hypercalcemia (TIH) amongst cancer patients in Pakistan.
Patients and Methods
The data were collected retrospectively. Cases of to have between consecutive patients who were reported hypercalcemia and admitted to the hospital January1988 and December 1997 were analyzed. Hypercalcemia was defined as a corrected serum calcium level of 10.6 mg/dl or more at presentation. Serum calcium level was corrected as under: for a fall in serum albumin of 1.0 gm/dI outside the reference interval (3.6-5 gm/dl; median 4gm/di), 0.8 mg/dl of calcium was added9.
The attending physician logged the medical diagnosis or to the face sheet of the medical chart. The medical records department used the international classification of diseases (lCD 9.0 version) coding system for indexing and coding of these records (275.4 - disorders of calcium metabolism).
Statistical Methods
The data are expressed as mean ± sd. The numerical variables were compared using Student’s t-test and categorical variables were compared using Pearson’s Chisquare test. Overall survival was calculated from the time of diagnosis of hypercalcemia to death or last follow-up.
Results
A total of 84 patients were diagnosed to have TIH. Similar numbers of episodes were evaluable.
The mean age at the time of presentation was 55± 14 years (17-85 years). There were 56 males and 28 females. Twenty five percent of the patients each had multiple myeloma and hepatocellular carcinoma whereas 20% of the patients had underlying breast cancer. The underlying diagnosis are shown in Table 1.

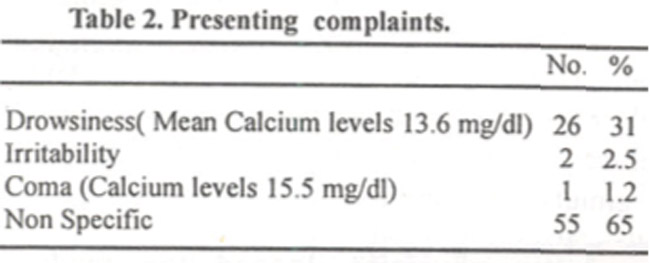
Almost one third of the patients presented with symptoms related to CNS dysfunction,whereas more than 65% presented with non-specific symptoms like nausea, vomiting, constipation etc. and other symptoms related to the underlying malignancy (Table 2).
The laboratory features at the time of presentation are shown in Table 3.
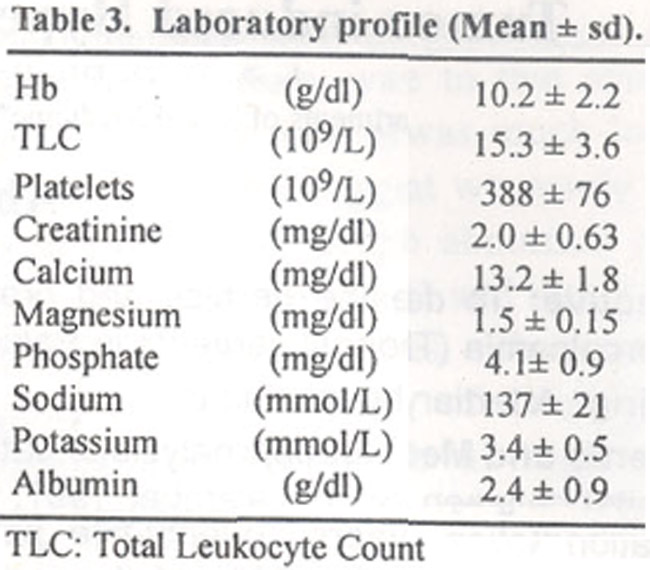
The mean hemoglobin was 10.2 ±2.2 gm/dl. The vast majority of patients had leukocytosis (5 8%) with a mean white cell count of 15.3 x 109/L. Serum creatinine was also elevated’ in the majority of patients. Sixty-nine percent of patients had serum creatinine level of more than 1.3 mg/dl (Normal reference range: 0.6-1.3). Eighty-six percent of patients had a serum albumin levels below the normal limits. Magnesium was also decreased in 47% of patients.
A total of 64 patients were evaluable for response to treatment. The other 20 (3 8%) patients died within the first 72 hours of diagnosis, before they could be evaluated for response. Of the 64 patients evaluable for response to treatment, twelve received intravenous normal saline and loop diuretics only, whereas, 34 also received corticosteroids. Four patients received subcutaneous calcitonin injections in addition to intravenous hyperhydration regimen. Fourteen patients were treated with bisphosphonates (6 with clodronate and 8 with pamidronate).
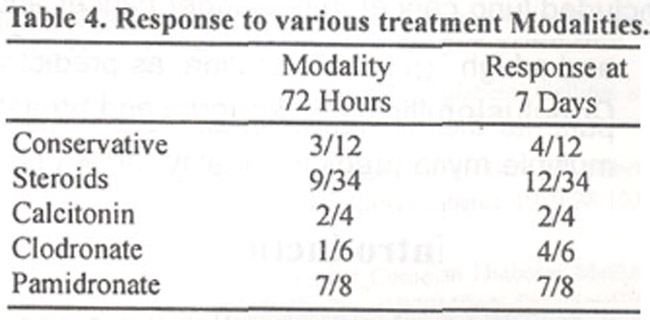
The response rates at 3 days and 7 days after initiating the treatment for each modality was recorded. Response was defined as resolution of CNS symptoms and a corrected serum calcium level of less than 10.6 mg/dl. Three and 4 out of 12 treated conservatively responded in 3 and 7 days respectively. Nine and twelve out of 34 treated with steroids responded in 3 and 7 days respectively. Eleven out of fourteen treated with bisphosphonates responded in 3 and 7 days. Two out of four patients responded with calcitonin at both 3 and 7 days. Details are shown in table 4.

A univariate analysis was performed to study various features at presentation, predicting early mortality (within 28 days). Age, presenting symptoms, hemoglobin, platelets, creatinine and albumin did not have an impact on the outcome. Male sex (p <0.04), underlying diagnosis other than multiple myeloma (p<0.025) and a high TLC (p <0.05) at presentation predicted an early mortality.
Discussion
TIH essentially occurs due to a marked increase in osteoclast-mediated bone resorption4. As many as 15% of patients with solid tumors, 20% patients with multiple myeloma, 80% of patients with adult T cell leukemias and 100% patients with advanced lung cancer may present with TIH3. The early symptoms of TIH are non-specific and the diagnosis is usually suspected when patients present with neurological symptoms such as lethargy, drowsiness, disorientation, stupor and coma. In our series one third of the patients presented with CNS symptoms. Once the diagnosis is established, treatment of TIH results in symptomatic improvement for a vast majority of patients. “Non-specific complaints” such as polyuria, polydipsia etc. improved in more than three-fourths of patients whereas the CNS symptoms also improved in more than two-third of the patients10. However, CNS symptoms were generally recorded and an assessment of clinical benefits of antihypercalcemia therapy could be made. Furthermore, we restricted the response criteria for this study as normalization of serum calcium levels.
Fifty eight percent of the patients had leukocytosis. The reason could be multifactorial. Concomitant infection, bone marrow involvement, use of steroids, etc. could explain leukocytosis. More recently some investigators have suggested that infiltration by cancer cells such as in multiple myeloma be another contributory factor. The secretion of hematopoietic growth factors such as G-CSF (Granulocyte Colony Stimulating Factor) or GM-CSF (Granulocyte-Monocyte Colony Stimulating Factor) by the tumor cells, may simultaneously act on osteoclasts and granulomonocytic cells11. Same study also suggested that tumors simultaneously produced both PTHrP and GCSF causing hypercalcemia and Leukocytosis11.
More than two-third of patients in our series had acute renal failure (ARF). Hypercalcemia leads to intravenous volume depletion and prerenal azotemia. Another potential precipitant of renal failure is the concomitant long-term use of non-steroidal anti-inflammatory agents. In one series, the incidence was shown to be 43%12
One of the limitations of this study was its retrospective nature; hence there was no control on the type of treatment modality chosen for a particular patient. The patients in the earlier part of the series received either normal saline only or steroids in addition to normal saline. It was only from 1994 onwards, that patients were treated with bisphosphonates. While comparing treatment modalities in terms of normalization of calcium levels, bisphosphonates were found superior to conservative treatment (with or without steroids). Of the patients who responded either completely or partially. there was a marked improvement on the neurological symptoms.
As shown in Table 4, the response to bisphosphonates was superior to the other treatment modalities. Bisphosphonates resulted in normalization of serum calcium within 72 hours in about sixty percent of the patients and the response was sustained over next several days.
Another limitation of this study is the paucity of long-term follow up on these patients. Long-term sustainability of response could not be evaluated because majority of these patients were either continued to be treated with other type of treatments including chemotherapy or hormone therapy or were lost to follow up after the treatment of hypercalcemia.
In conclusion, multiple myeloma, hepatoma and breast carcinoma were common cancers associated with TIH. One-third of the patients died within first few days. Male sex, underlying diagnosis other than multiple myeloma and a high total leukocyte count suggested an unfavorable outcome. Bisphosphonates reduced calcium levels within 7 days in more than 75% of patients.
References
1.Fallon MT. Hanks OW. Control of common symptoms in advanced cancer. Ann. Acad. Med. Singapore, 1994;23: 171-7.
2.de Ia Mata J, Uy HL, Guise TA, et al. Interleukin-6 enhances hypercalcemia and bone resorption mediated by parathyroid hormone-related protein in vivo. J. Clin. Invest., 1995; 95: 2846-52.
3.Lee JK, Chuang Mi, Lu CC, et al. Parathyroid hormone and parathyroid hormone related protein assays in the investigation of hypercalcemic patients in hospital in a Chinese population. J. Endocrinol. Invest., 1997; 20: 404-9.
4.Body JJ. Medical treatment of tumor-induced hypercalcernia and tumor-induced osteolysis: challenges for future research. 5upport-Care-Cancer, 1993; 1: 26-33.
5.Body JJ, Dumon JC. Treatment of tumour-induced hypcrcatcaemia with the bisphosphonate pamidronate: dose-response relationship and influence of tumour type. Ann. Oncol., 1994; 5: 359-63.
6.Coleman RE. Skeletal complications of malignancy. Cancer, 1997; 80: 1588-94.
7.van Holten Verzantvoort AT, Papapoulos SE. Oral pamidronate in the prevention and treatment of skeletal metastases in patients with breast cancer. Medicina B. Aires, 1997;57: 109-13.
8.Usui 1, Oiso Y, Tomita A, et al. Pharmacokinetics of incadronate, a new bisphosphonate, in healthy volunteers and patients with malignancy-associated hypercalcemia. tnt. J. Clin. Pharmacol. Ther., 1997; 35:239-44.
9.Walmsley RN, White GH. Calcium, Magnesium and Phosphate. In: A guide to diagnostics clinical chemistry (Third eds). Osney Mead, Oxford, OX2 0EL. Blackwell Scientific Publications; 1994, pp. 178-221.
10.Rolston Ky. Management of febrile episodes during neutropenia caused by chemotherapy. Am. J. Clin. Oncol., 1990;13: 171-4.
11.Kato N, Yasukawa K, Onozuka T, et at. Paraneoplastic syndromes of leukocytosis, thrombocytosis, and hypercalcemia associated with squamous cell carcinoma. J Dermatol., 1999; 26:352-8.
12.Irish AB, Winearls CG, Littlewood T. Presentation and survival of patients with severe renal failure and myeloma. Q. J. Med., 1997; 90: 773-80.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: