
Manzoor Hussain ( Sindh Institute of Urology and Transplantation (SIUT), Karachi. )
Murli Lal ( Sindh Institute of Urology and Transplantation (SIUT), Karachi. )
Syed Hasan Askari ( Sindh Institute of Urology and Transplantation (SIUT), Karachi. )
Altaf Hashmi ( Sindh Institute of Urology and Transplantation (SIUT), Karachi. )
Syed Adibul Hasan Rizvi ( Sindh Institute of Urology and Transplantation (SIUT), Karachi. )
October 2010, Volume 60, Issue 10
Original Article
Abstract
Objective: To evaluate the efficacy and long-term results of laser urethrotomy as minimally invasive treatment for traumatic stricture urethra.
Methods: Between January 2006 and June 2008, 78 male patients were treated with Holmium Laser urethrotomy. 16 Fr urethroscope was used through which 600um laser fiber was introduced through side channel. Stricture was visualized and incised at 12 o\'clock position with energy set at 1500-2000 MJ at pulse rate of 10-12. Two other incisions were given at 2 and 10 o\'clock positions. Further ablation was done till 16Fr Foley\'s catheter was passed. Patients were followed in a stricture clinic.
Results: Patients age ranged from 15-73 years. All strictures were due to trauma, Road traffic accident in 40(52%) post catheter trauma 4(5%), fall as ride 27(35%) and failed urethroplasty 7(8%). Site of stricture was bulbar 57(73%), bulbomembranous 16(20%) and membranoprostatic 5(2.5%). Length of stricture ranged from 0.8-2.5 cms.
At 3 months follow-up, 60(77%) patients remained catheter and symptoms free while 18(23%) developed recurrence of stricture but at the end of 36 months follow-up success rate decreased to 47 (60%). Among those who developed re-strictures, 6(7.6%) had 2nd sitting laser while 4(5.1%) had urethroplasty, and others were on intermittent dilatation. Immediate complications were sepsis 10(13%), extravasation 2(4%), failed urethrotomy 2(4%) and mild haematuria 3(5.8%). Hospital stay ranged from day care to 3days.
Conclusion: Laser urethrotomy is minimally invasive and an effective treatment for short strictures in bulbarurethra. The recurrence rate is 40% in the long-term follow-up and is more commonly seen in completely obliterated strictures (JPMA 60:829; 2010).
Introduction
Stricture urethra constitutes 3-4% of urologic workload at our Institute and the main causative factor is trauma.1 Urethral dilatation has remained the treatment for this disease at our stricture clinic since 1972. How ever in 1990, Direct vision internal urethrotomy (DVIU) was introduced at SIUT and till 2008, seven hundred and twenty-six (726) such procedures have been performed. The complications associated with internal urethrotomy include bleeding, UTI, Urosepsis, extravasation, incontinence, impotence and recurrence of stricture.2 Excision and primary anastomotic urethroplasty is the gold standard in the management of traumatic stricture urethra but has higher complication rates like bleeding, impotence, infertility and in some cases failure and recurrence of the stricture.3 Also hospital stay is longer and indwelling catheter time is prolonged. Therefore, several alternative approaches have been evaluated in the management of traumatic stricture urethra. The first laser used for urethrotomy was by Bulow H4 in 1979. After this few studies have been published on the use of lasers in strictures with varying techniques.5 The objective of the present study was to evaluate the outcome of Holmium YAG-laser urethrotomy performed at our institute in terms of safety, efficacy, complications and long term results in the management of traumatic stricture urethra.
Patients and Methods
From January 2006 - June 2008, seventy-eight male patients with traumatic stricture urethra were treated using holmium laser urethrotomy at our Institute. Pre-operative evaluation included history, physical examination, combined retrograde urethrogram, (RUG) and voiding cystourethrogram (VCUG), urine culture sensitivity and urethroscopy.
Patients with other causes of stricture in whom laser was used were excluded from this study.The length of stricture was evaluated by a measuring scale on voiding and retrograde urethrogram.
Technique of Laser urethrotomy:
The Laser machine used in this study was Holmium YAG-laser Auriga Starmedtec Germany. All 78 patients underwent the procedure under general anaesthesia. Patients with positive urine cultures were initially treated with antibiotics, whereas those with negative urine culture received prophylactic antibiotics pre-operatively. The patient was placed in lithotomy position and urethroscopy was performed with 17 FR scope with zero degree lens. Under vision, laser incision was given at 12 o\'clock position, with 600 m fiber energy set at 1500 - 2000 mJ and frequency of 12 Hz. After the initial incision at 12 o\'clock, a circumferential ablation of stricture was done and cutting continued till normal urethra was visualized proximally. Thereafter 16 FR Foleys catheter was retained for 5 days in most of the patients. They were then called for follow up in the stricture clinic where the catheter was removed. If the patient passed urine voluntarily, uroflowmetry was done. Follow-up of these patients was extended up to September 2008, UFM was done at 3, 6 months and at the end of study. Statistical analysis was performed using SPSS-10.
Criteria used for Assessment:
Excellent results were defined as catheter free, improvement in symptoms and Q-max more than 15 ml/sec.
Re-stricture formation was defined as recurrence of retention of urine, need for another procedure, or Q-max less than 10 ml/sec.
Results
The age of patients ranged from 15 - 73 years with mean age of 34.7 ± 9. The various causes of trauma included road traffic accident (RTA=40 (51.3%), fall astride=27 (35%), failed urethroplasty 7 (8%), post catheter 1 (1.2%) and post TURP 3 (3.8%). The commonest site of stricture was bulbar urethra in 57 (73%), out of these 7 patients had multiple strictures, 16 (20%) had bulbomembranous stricture and membraneo prostatic in 5 (6.5%) cases. The length of strictures ranged from 0.8 to 2.5 cms in this series but 44 (56.4%) patients had stricture length of 1 -2 cms (Table-1).
Thirty-seven patients (47.4%) had history of previous treatment, cold knife urethrotomy 7 (8.9%), rail road catheterization 1 (1.2%), TURP 3 (3.8%), Urethroplasty 7 (8%) and urethral dilatation in 19 (22%).
Out of 78 traumatic strictures, laser urethrotomy was possible in 76 cases. In 2 (2.5%) patients laser treatment failed because of total obliteration of posterior urethra. Immediate and post-operative complications were seen in 17 patients (Table-2). UTI with or without signs and symptoms of sepsis (shivering, fever, increased TLC, positive urine culture) was the most frequent complication seen in 10 (13%) patients. Other minor complications are shown in Table-2.
Analysis at 3 months of follow-up showed excellent results in 60 (77%) cases but at 6 months follow-up, 7 more patients developed re-stricture formation and at the end of study period (at 36 months) the success rate decreased to 47 (60%) patients, so the success rate at mean follow-up of 15.8+10.3 months was 60% (Table-3). Thirty-eight (49%) patients were treated as day care cases while 32 (41%) remained hospitalized for 24 hours for logistic reasons and only 8 (10%) patients remained admitted for 2-3 days. Mean hospital stay was 21.8 ± 14.7 hours (Table-2). Laser operation time ranged from 3 -60 minutes with mean of 26.2 ± 14.1 minutes. Post-operative duration of catheterization ranged from 2-15 days with mean of 5 ± 1.7 days. The follow-up of these patients ranged from 3-36 months with mean 15.8 ± 10.3 months.
At mean follow-up of 15.8 ± 10.8 months, a total of 31 (40%) patients developed recurrence of stricture at the previous site which was less severe than the original stricture length. These were treated by various methods. Six received a second sitting of Laser Urethrotomy, 4 had Urethroplasty and 21 patients were managed with intermittent dilatation. The relationship of stricture free rate and follow-up in months is shown in Figure.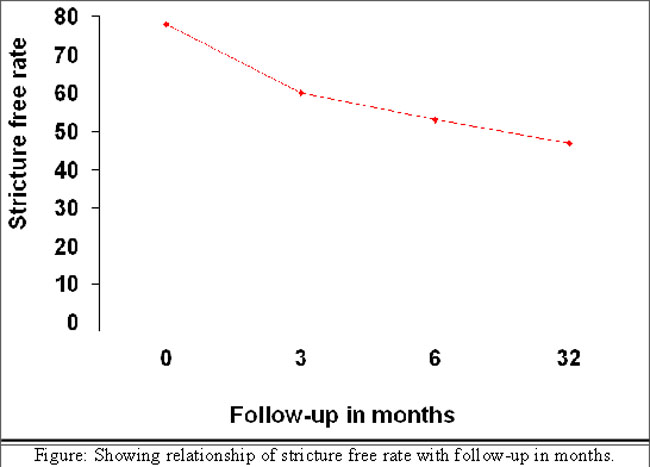
Pre-operative uroflowmetry (UFM) ranged from 0 - 7 ml/sec with a mean of 0.9 ± 1.7 ml/sec while on post-operative follow-up UFM ranged from 11-28 ml/sec with a mean of 19.6 ± 4.1 ml/sec, Similarly pre-operative urinary tract infection were seen in 27 (36.6%) patients while on post-operative follow-up only 6 (7.6%) patients had positive urine culture (Table-3).
The success rate versus site and length of stricture is given in Table-1.
Discussion
The effective and safe management of traumatic stricture urethra has long been the dream of urologic surgeons and their patients. Recently several lasers have been used for stricture urethra ranging from Diode Laser, KTP Laser, Nd: YAG and Holmium YAG-laser with varying results.6,7 The apparent advantages of holmium laser are less bleeding, clear vision, precise incision and ablation of scar tissue and short hospital stay.3 To our knowledge this is the largest series on the use of Holmium YAG-Laser in the treatment of traumatic stricture urethra. An earlier study, from India reported the use of laser core through urethrotomy in 65 cases,8 but the present series includes 78 patients. Another series from Germany reported on 32 patients, with most being iatrogenic, only few were traumatic.9
The post-operative complications in our cases were seen in 20.5% of cases. All were minor in nature, as three patients had bleeding during the procedure which was treated by coagulating the vessel immediately with laser. Later on no secondary haemorrhage was encountered and no blood transfusion was needed in any case. This was in agreement with the study by Kamp S et al.9 Extravasation of irrigating fluid was observed in 2 (2.5%) patients in the initial period of the study which was treated by giving free incisions and placing a supra pubic catheter. After this experience we continued to observe the external genitalia during the procedure and avoided deep ablation in the bulbar urethra. Post-operative fever was observed in 10 (13%) of the patients inspite of pre-operative and post-operative antibiotics. Three of them had symptomatic uro-sepsis which was treated by intravenous antibiotics, hydration and supportive therapy. Kamp S et al9 reported post-operative urinary tract infections in 5% cases. In the present series the higher incidence of UTI and sepsis could be due to more complex strictures with supra pubic catheter in situ and history of multiple procedures in the past. The mean operation time was 26.2 ± 14.1 minutes in this series with a range of 3-60 minutes, We observed that with a longer laser time, septic complications (fever, shivering) were more frequent and patients complained of urethral burning pain if the laser time was more than 15 minutes.
In this study, excellent results were seen in 60 out of 78 (77%) cases at 3 months. These were defined as catheter free status with Q-max more than 15 ml/sec and no requirement for any other intervention. The follow-up period ranged from 3 to 36 months with a mean of 15.8 ± 10.3 months. Kamp S et al9 reported good results in 70% of their cases at 27 months follow-up, while Dogra et al8 from India reported excellent results in 74% at mean follow-up of 30 months. Our results confimed the findings quoted in the previous reports. In our study 31 (40%) patients had recurrence of stricture at the end of follow-up. The analysis of this group showed that all were completely obliterated strictures and long segment strictures (more than 1.5 cms in length) and had history of previous procedures like optical internal urethrotomy or dilatation. In our study it was observed that the best success rates were had in bulbar strictures with shorter length similar to the study by Kamp et al.9 Matsuka et al10 reported restricture formation in 35% cases after laser urethrotomy. The patients were treated either with re-incision or urethral dilatation similar to our series.
Conclusion
Laser urethrotomy is minimally invasive and an effective treatment for short strictures in the bulbar urethra while posterior urethral strictures and patients with history of previous procedures, are likely to have restricture formation in long-term follow-up.
Acknowledgement
I am grateful to Dr. Fatema Jawad for reviewing and correcting the manuscript editorially. I am also thankful to Mr. Shamshad Hussain for secretarial help.
Reference
1.Hussain M, Hamid R, Soomro S, Hashmi A, Naqvi S.A.A and Rizvi S.A.H. Pattern and management of genito urinary trauma in a tertiary care centre in Pakistan: Analysis of 450 cases. J NUT 2002; 3: 6-10.
2.Santucci RA, Jayee GF, Wise M. Male urethral stricture disease. J Urol 2007; 177: 1667-74.
3.Hussain M. Urethral stricture disease: An old disease with newer treatments. J. Pak Med Assoc 2008; 58: 227-8.
4.Bulow H, Bullow U, Frohmullar HW. Transurethral laser urethrotomy in man: Preliminary report. J Urol 1979; 121: 286-7.
5.Turek PJ, Malloy TR, Cendran M, Carpiniello VL, Wein AJ. KTP-532 laser ablation of urethral stricture. Urology 1992; 40:330-4.
6.Kamel BA. The use of diode laser for treating urethral strictures. BJU Int 2001; 87: 831-3.
7.ShanBerg A, Bagholassarian R, Tansey L. Sawyer D. KTP 532 Laser in the treatment of urethral strictures. Urology 1988; 32: 517-20.
8.Dogra PN, Nabi G. Core through urethrotomy using the Neodymium: YAG laser for obliterative urethral strictures after traumatic utrethral disruption and or distraction defects: long term outcome. J Urol 2002; 167: 543-6.
9.Kamp S, Knoll T, Osman MM, Kohrmann KU, Michel MS, Alken P. Low-power Holmium: YAG Laser urethrotomy for treatments of urethral strictures: Functional outcome and quality of life. J Endourol 2006; 20: 38-41.
10.Matsuka K, Inoue M, Ilda S, Tomiyasu K, Noda S. Endoscopic antegrade laser incision in the treatment of urehral stricture. Urology 2002; 60: 968-72.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: