
Tanweer Iqbal ( Department of Nephrology, Sindh Institute of Urology and Transplantation Karachi, Pakistan. )
Rubina Naqvi ( Department of Nephrology, Sindh Institute of Urology and Transplantation Karachi, Pakistan. )
Syed Fazal Akhter ( Department of Nephrology, Sindh Institute of Urology and Transplantation Karachi, Pakistan. )
October 2010, Volume 60, Issue 10
Original Article
Abstract
Objective: To determine the risk factors of urinary tract infection in renal transplant recipients and its effect on graft function among transplanted patients visiting the outpatients department of Sindh Institute of Urology and Transplantation.
Methods: This cohort study was conducted at Transplantation department, Sindh Institute of Urology and Transplantation Karachi. The period of the study enrollment extended from April 2008 to September 2008 Included were two hundred adult live related renal transplant recipients who were enrolled during the initial post transplant period and followed up for one year. Analysis was done by using SPSS ver 10.0. The level of significance was taken as 0.05. Student\'s t test and chi square test were used to compare the variables in both groups.
Results: The mean age of the patients was 30± 10 years. Sixty six (33%) renal transplant recipients had at least one episode of urinary tract infection which occurred in 51 (77%) patients during the first two months after renal transplant and 8 (12%) patients had recurrence of infection. Gram negative bacilli were the principally isolated agents. E. coli was found in 34 (51%) patients and Pseudomonas in 12 (18%). Renal stone disease, structural abnormalities, delays in Foleys removal, and post operation hospital stay were statistically significant risk factors for urinary tract infection in the patients. Twenty three recipients of the study developed early graft dysfunction due to urinary tract infection. No graft was lost in either groups.
Conclusion: Structural abnormalities, renal stone disease, delay in removal of Foley\'s catheter and increased post transplant hospital stay are risk factors leading to UTI in renal transplant recipients (JPMA 60:826; 2010).
Introduction
Urinary tract infection (UTI) is the single most important bacterial infection in renal transplant recipients and it remains a major problem despite advances in organ transplantation.1 The frequency of UTI varies from 30-79% in different studies with approximately 60% of bacteraemia originating from this site.2 Sqalli et al reported 42% patients developing UTI,3 while Hussain et al demonstrated UTI in 46% recipients.4 The primary goal in organ transplantation is the achievement of good graft function simultaneously prevention and effective treatment of infections.5
Occurrence of UTI depend on many factors such as age, female gender, co-morbidity, type and amount of immunosuppression, urological instrumentation and/or length of follow up period after kidney transplantation.6,7 UTI may have an adverse impact on graft and patient\'s survival. Other factors such as indwelling catheter, handling and trauma to the kidney and ureter during surgery, structural abnormalities of the native or transplanted kidneys, neurogenic bladder, renal insufficiency, and possible rejection may also explain the high incidence of UTI in renal transplant recipients.8,9 The typical micro-organisms causing post transplant UTI are enteric gram negative bacilli and enterococci, in addition Corynebacterium urealyticum of group D2 has been identified as a potential pathogen.10,11
To the best of our knowledge there is only one retrospective study on UTI in renal transplant recipients in Pakistan,12 therefore this study will help to determine the specific risk factors which can lead to UTI in renal transplant recipients and its effect on graft function.
Patients and Methods
This study was conducted at Sindh Institute of Urology and Transplantation (SIUT) Karachi, Pakistan to determine risk factors of UTI in live related renal allograft recipients and its effect on graft function. It was a cohort study conducted for 18 months enrolment period commencing from April 2008 to September 2008. All adult recipients were included consecutively irrespective of their gender and primary cause of renal dysfunction. Recipients less then 18 years of age were excluded from this study. Two hundred adult recipients were enrolled during initial post transplant period and followed up weekly for first two months then fortnightly for another two months and monthly for total one year through out patient\'s department. No patient was lost during follow up in this study. In all transplanted patients surgical technique was standard. The kidney graft was placed extraperitoneally in the right iliac fossa, the renal artery was anastomosed to the internal iliac or external iliac artery, and the vein to the external iliac vein. The ureter was anastomosed to the recipient bladder using Lich-gregoire technique. The immunosuppression for most patients consisted of triple regimen including cyclosporine, Azathioprine, prednisolone and rejection episodes were treated with pulse methyl prednisolone. In the case of steroid resistant rejection, Anti-thymocyte globulin were used. Urinary culture was obtained atleast once a week while the patient was in hospital after the transplantation. In out patient clinic, on every visit serum Creatinine and urine D/R was checked, and cultures were taken when there was significant WBC count in urine D/R, symptoms of urinary tract infection were present, or when the patient was febrile or in asymptomatic patients presenting with rise in serum Creatinine. Patients with positive urine culture and graft dysfunction were treated for six weeks whereas those with positive culture but no graft dysfunction received treatment for three weeks. All patients received sulfadoxine-pyrimethamine prophylaxis for Pneumocystis carinii pneumonia and UTI for one year.
UTI was defined as urine culture containing more than 105 colonies.3 Graft dysfunction was defined as more than 20% rise in serum Creatinine after diagnosing UTI.
Various factors which can cause UTI were studied. Major emphasis was placed on age and sex, primary disease which caused renal failure, the effect of Foleys catheter, presence of double J stent, the effect of immunosuppression as well as rejection therapy and the effect of UTI on graft function. Also studied were the organisms prevalent among transplant patients causing UTI, their pattern of sensitivity and resistance and effect of antibiotic therapy. The effect of UTI on graft function and one year graft survival was also calculated in these patients.
Data regarding age, gender, cause of primary disease, immunosuppression protocol, type of anti rejection therapy, type of ureteroneocystostomy, number of days Foleys catheter was retained, presence of double J stent, infective organism and graft dysfunction was collected through a questionnaire. This data was entered in Statistical Package for Social Sciences Version 10.0. Student\'s t test and chi square test were used to analyze different factors for the two groups made on the basis of the presence or the absence of UTI. A p value less than 0.05 was considered as significant.
Results
Two hundred patients comprising of 168 men and 32 women with a mean age of 30 ± 10 years who underwent live related renal transplant were reviewed during hospitalization and in the out patient department. It was the first transplant for 197 patients while 3 patients had a second transplant. The patient\'s characteristics are shown in Table-1.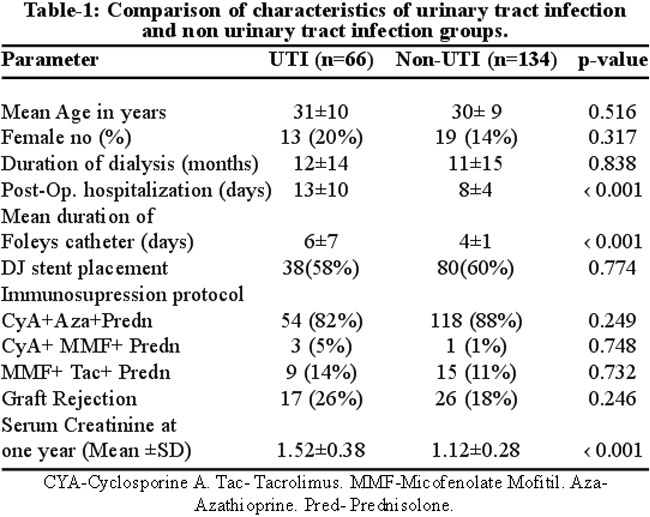
The underlying causes for End Stage Renal Failure in the patients of the original renal disease in renal transplant recipients included stone disease in 34 (17%), glomerulonephropathy in 10 (5%), hypertensive nephropathy in 14 (7%), diabetic nephropathy in 8 (4%), adult polycystic kidney disease in 6 (3%), and unknown cause in 128 (64%) patients.
Fiftythree males and 13 females suffered at least one UTI episode. UTI was more common in age range of 18-29 years. No symptoms were reported by 29 (44%) patients on presentation while 29 (44%) had febrile illness and 8 (12%) had dysuria and flank pain. Double J stent was placed during surgery in some patients to prevent leakage of urine and ureteric stenosis. Thirty eight (58%) out of 66 patients with a stent developed UTI, while 80 (60%) out of 134 had a stent placement but no UTI. No significant difference was found between both groups (p=0.774). Time of occurrence of infections after transplant was also important. Infections during the first six months had significant impact on graft function. In the study patients, UTI episodes occurred in 51 (77%) during the first two months post renal transplant with a recurrence rate of 12%.The causative micro-organisms of UTI are shown in Table-2.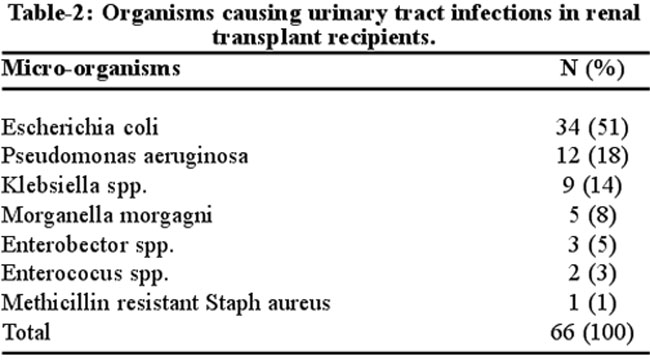
Fifty (76%) patients responded to antibiotic therapy, while sixteen (24%) showed partial response. Micro-organisms resistant to broad spectrum antibiotic (MDR) were found in the urine of 5 (7%) recipients, and Pseudomonas was the most frequent organism (n=3). The mean serum Creatinine before UTI was 1.35 ± 0.39 mg/dl while after developing UTI, it increased to 1.74 ± 0.96mg/dl. After treatment serum Creatinine declined to 1.37 ± 0.43 mg/dl.
In the study population, 34 patients had stone disease, of whom, 20 (59%) developed UTI (p=0.001). Four patients had structural abnormalities of the urinary tract and all of them developed UTI (p= 0.004). Post transplant hospital stay (p=‹0.001) and delay in removal of Foleys catheter (p=‹0.001) were also found to be statistically significant factors causing urinary tract infection in our transplant population. Twenty three (35%) patients developed early graft dysfunction with UTI, in addition urinary tract infections did not increase the risk of graft loss.
Discussion
Structural abnormalities, renal stone disease, delay in removal of Foleys catheter and increased post transplant hospital stay were statistically significant factors leading to urinary tract infection in the presented study on renal transplant recipients.
As with the general population, it was discerned that structural abnormalities increased the risk for developing urinary tract infections in renal transplant recipients.13 In this study on renal transplant population, patients with structural abnormalities (reflux uropathy, bladder outlet obstruction) developed UTI.This is consistent with the results of Chuang et al14 and Sqalli et al3 who reported a high incidence of UTI in patients with structural abnormalities. Renal stone disease increases the relative risk for developing UTI in renal transplant recipients. To the best of our knowledge renal stone disease has not been identified as a significant risk factor for UTI among renal transplant recipients. This is partly due to a high prevalence of stone disease along with as late presentation and incomplete treatment leading to end stage renal disease in this region whereas in other regions it is the opposite.15,16
In addition to structural abnormalities and renal stone disease we observed several other patient characteristics to be independently associated with urinary tract infections in the renal transplant population. Recipients who had prolonged Foleys catheterization and increased post transplant hospitalization were found to have an increased risk of developing UTI in this cohort.of transplant recipients. These findings were consistent with study by Dantas et al. which also demonstrate the length of hospitalization before the infection and duration of urinary bladder catheterization as main risk factors for urinary tract infections in post transplant patients.17
Female transplant patients have been reported to have a higher risk of developing UTI than men after renal transplantation.11,18 The reason might be the difference in anatomical construction (shorter urethra and proximity of the urethral opening to the vagina and anus) in female patients. In the study of Chuang et al14 68% of female transplant patients in comparision to 30% of male transplant patients had at least one UTI post transplant. On the other hand Dantas et al17 did not find any sex related difference in their study. In our study 35% of female transplant recipients against 32% of male transplant recipients had urinary tract infection which was not statistically significant, the reason could the small number of female patients in our study.
Diabetic nephropathy has also been widely reported to be associated with increased risk of UTI.7 This was not observed in our study with no significant association between pre transplant diabetes and increased risk of urinary tract infection. This could be due to the small number of diabetic patients in the study group. Other causes of end stage renal disease were not found to be a significant cause for increasing the risk of post transplant urinary tract infections in our renal transplant recipients.
Most UTI episodes occur during the first three months post transplantation.19,20 An earlier study from SIUT reported UTI in 65% recipients in the first three months of post transplantation4 Similarly Renoult et al reported UTI in 74% of patients during first month after kidney transplantation.19 The present study conforms with the past finding with 77% UTIs occurring in first two month after renal transplant.
The most frequent organisms demonstrated in transplant recipients were Escherichia coli and other gram negative bacteria, such as Klebsiella spp., Enterobector spp, and Pseudomonas aeruginosa.19,21 A regional study by Sharma et al demonstrated E. coli as a common isolate followed by Staphylococcus, Enterococus and Pseudomonas.22 We also found E. coli as a leading cause of UTI, followed by Pseudomonas, Klebsiella, Morganella morgagni. At one year post transplant, 35% recipients with UTIs had graft dysfunction as compared to non UTI group. No recipient had graft loss in both groups at the end of the study which is similar to a study conducted by Chuang et al.14
Conclusion
There are conflicting data on the association of post transplant urinary tract infections with graft and patient survival, with predisposing factors varying in different centers world over. It is also agreed upon that prolonged infections pose extra risk on graft survival.
In our renal transplant recipients, structural abnormalities, renal stone disease, delay in removal of Foleys catheter and prolonged hospitalization in the post transplant period are significant risk factors for development of UTI.
References
1.Satish R, Gokulnath. Intractable urinary tract infection in renal transplant recipients. Saudi J Kidney Dis Transpl 2009; 20: 458-61.
2.Brayman KL, Stephanian E, Matas AJ, Schmidt W, Payne WD, Sutherland DE, et al. Analysis of infectious complications occurring after solid organ transplantation. Arch Surg 1992; 127: 38-48.
3.Sqalli TH, Laboudi A, Arrayhani M, Benamer L, Amar Y, Ouzeddoun N. Urinary tract infection in renal allograft recipients from living related donors. Saudi J Kidney Dis Transplant 2008; 19: 551-53
4. Hussain Z, Rizvi SAH, Naqvi A, Zafar N, Ahmed E, Sultan S. Risk factors and adverse effects of urinary tract infections in live related allograft recipients. Am J Tran 2003; 507 Abs. 1385 poster board session: p141-111.
5.Jay A, Fishman MD, Robert H, Robin MD. Infection in organ transplant recipients. N Eng J Med 1998; 38: 24.
6. Saemann M, Hori HI. Urinary tract infection in renal transplant recipients. Eur J Clin Inves 2008; 38: 58-65.
7.Takai K, Tollemar J, Wilezek HE, Groth CG. Urinary tract infection following renal transplantation. Clin Transplant 1998; 12: 19-23.
8.Wilson C, Bhatti A, Rix D, Manas D. Routine intraoperative ureteric stenting for kidney transplant recipient. Cochrane Database Syst Rev 2005; 4: CD 004925.
9.De Souza RM, Olsburgh J. Urinary tract infection in renal transplant patients. Nat Clin Pract Nephrol 2008; 4: 252-64.
10.Aquado JM, Salto E, Morales JM, Munoz MA, Lizasoain M, Lumbreras C, et al. Corynebacterium urealyticum: A new and threatening pattern for the renal transplant patients. Transplant Proc 1993; 25: 1493-4.
11.Domann E, Hong G, Imirzalioglu C, Turschner S, Kuhle J, Watzel C, et al. Culture independent identification of pathogenic bacteria and polymicrobial infection in the genitourinary tract of renal transplant recipient. J Clin Microbial 2003; 41: 5500-10.
12.Rizvi SAH, Naqvi SAA. Renal transplantation in Pakistan. In: Cecka MJ and Terasaki PI eds. Clinical Transplants. UCLA Immonogenetics Center, Los Angels, 2000: 381-2.
13.Erturk E, Burzon DT, Orloff M, Rabinowitz R. Outcome of patients with vesicoureteric reflux after renal transplantation: The effect of pre transplantation surgery on post transplant urinary tract infection. Urology 1998; 51: 27-30.
14.Chuang P, Parikh CR, Langone A. Urinary tract infections after renal transplantation: A retrospective review at two US transplant centers. Clin Transplant 2005; 19: 230-5.
15.Rizvi SAH, Naqvi SAA, Hussain Z, Hashmi A, Hussain M, Zafar MN et al. the management of stone disease. BJU International 2002; 89 (Suppl .1): 62-8.
16.Olafur SI, Sigurjan B, Vidar OE, Helgi S, Nikulas S, Runolfer P. Epidemiology of kidney stones in Ice Land: A population based study. Scand J Urol Nephrol 2006; 40: 215-20.
17.Dantas SR, Kuboyama RH, Mazzali M, Moretti ML. Nosocomial infections in renal transplant patients: Risk factors and treatment implications associated with urinary tract and surgical site infections. J Hosp Infect 2006; 63: 117-23.
18.Maraha B, Bonten H, Van Hooff H, Fiolet H, Buiting AG, Stobberingh EE. Infectious complications and antibiotic use in renal transplant recipients during a 1 year follow up. Clin Microbial Infect 2001; 7: 619-25
19.Renoult E, Aouragh F, Mayeux D, Hestin D, Lataste A, Hubert J, et al. Factors influencing early urinary tract infections in kidney transplant recipients.Transplant Proc 1994; 26: 2056-8.
20.Khosroshahi HT, Mogaddam AN, Shoja MM. Efficacy of high dose trimethoprim-sulfamethoxazol prophylaxis on early urinary tract infection after renal transplantation. Transplant Proc 2006; 38: 2062-4.
21.Takai K, Tollemar J, Wilczek HF, Groth CG. Urinary tract infections following renal transplantation. Clin Transplant 1998; 12: 19-23.
22.Sharma KK, Ayyagiri A, Dhole TN, Prasad KN, Kishore J. prevalence of infection in renal transplant recipients of north India. Indian J Pathol Microbiol 2007; 5: 453-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: