
Moinuddin Khan ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Faisal Qadir ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Bashir Hanif ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Bilawal Ahmed ( Medical Student, Dow University of Health Sciences, Karachi, Pakistan. )
Arif Valliani ( Medical Student, Dow University of Health Sciences, Karachi, Pakistan. )
October 2010, Volume 60, Issue 10
Original Article
Abstract
Objective: To determine the safety and success of transradial coronary angiography and angioplasty in a Pakistani population.
Methods: This was a prospective study on 264 consecutive patients undergoing transradial coronary angiography (TRCAG) and angioplasty (TRCAP) at Tabba Heart Institute, Karachi between November to December 2008. All patients enrolled in the study underwent Allen\'s test to ensure dual arterial supply to the hand. Modified Allen\'s test was performed only when Allen\'s test was abnormal. Patients were excluded from the study if they had abnormal Allen\'s and modified Allen\'s test, were on haemodialysis or had abnormal serum creatinine level. The main outcome measures were success rate and complications of TRAG and TRCAP.
Results: The mean age was 57 ±11.08 years with 199 (75.4%) males and 64 (24.6%) females. A total of 182 (76.3%) coronary angiographies and 82 (76.8%) coronary angioplasties were preformed from the trans-radial route in the study period. Overall procedural success rate was 94% for TRCAG with mean procedure time of 23.74 ± 6.26 minutes and mean fluoroscopy time of 5.65 ± 2.3 minutes. The success rate for TRCAP was 93.6% with mean procedure time of 62 ±10.6 minutes and mean fluoroscopy time of 15.78 ± 8.90 minutes. Only 1 patient had mild forearm haematoma and asymptomatic radial artery occlusion occurred in 4 (1.5%) study patients.
Conclusion: Trans-radial artery cannulation is a safe and successful route for performance of coronary procedures. It can be used as an acceptable alternate to transfemoral approach (JPMA 60:809; 2010).
Introduction
Common femoral artery (CFA) has traditionally been the site of access for coronary angiography and angioplasty. The size of femoral artery has been the key factor in preferring this site for access, especially in the era of large diameter diagnostic and angioplasty guiding catheters and poor profile balloons. The availability of better coronary equipment and newer anticoagulation agents has broadened the horizon for coronary interventions. The CFA approach for coronary interventions could be complicated by serious vascular access site complications including haematomas accompanied by significant blood loss, arterial pseudoaneurysm and arteriovenous fistulas. Bleeding from vascular access site is by far the most feared complication especially with use of anticoagulation and platelet Glycoprotein IIb/IIIa inhibitors. The overall incidence of major bleeding was 3.9% in the GRACE1 registry, out of that vascular access site bleeding occurred in 23.8% and retroperitoneal bleeding in 6% of patients undergoing angioplasty in the setting of acute coronary syndrome from transfemoral approach. The in hospital mortality was significantly higher in patients with major bleeding than in those without major bleeding (18.6% vs 5.1%).
In 1989 Campeau first reported the result of transradial angiography (TRCAG) with 5F catheter in 100 patients with a success rate of 88% without any access site complications.2 Later the work by Kiemeneij in angioplasty through transradial route3 has attracted the interventionist worldwide. In comparison to transfemoral route, major vascular access site complications are minimized from radial artery approach, even with concomitant use of high doses of anticoagulation and Glycoprotein IIb/IIIa platelet inhibitors(0% vs 7.4%).4 Coronary interventions from transradial route in acute myocardial infarction have been shown to be extremely safe. Transradial route has demonstrated similar success rate with no major access site complications compared to 5.5% in transfemoral group in patients undergoing primary angioplasty.5 Compared to 13% access site complications from femoral artery in rescue PCI, transradial route had 0% complications with similar success rate.6 The other advantages have been improvement in patient comfort; early ambulation and shorter hospital stay.7
Despite these advantages, the radial artery is accessed in less than 10% of coronary procedures globally.8 Asian population, especially Asian females tend to have small caliber radial artery because of small body habitus,9 which could make this route more challenging. There is no data available regarding the trans-radial route of angiography and angioplasty in Pakistani population as only limited centers are using radial artery for these procedures. This study is aimed to determine the procedural safety and success of trans-radial angiography and angioplasty in a Pakistani population.
Patients and Methods
This was a prospective study conducted on 264 consecutive patients undergoing transradial coronary angiography (TRCAG) and angioplasty (TRCAP) at Tabba Heart Institute, Karachi between November to December 2008. Written informed consent was taken from all patients and the study protocol was approved by the hospital ethical review committee.
Patients of both genders and all ages who were either admitted in the hospital or were admitted in the day care unit for angiography or angioplasty were included.
Indications for coronary angiography and angioplasties were acute coronary syndrome, significant symptomatic angina, abnormal stress test or myocardial perfusion scan. All selected patients underwent routine history and clinical examination along with assessment of dual arterial supply to both hands by performing Allen\'s test. Modified Allen\'s test was performed only when Allen\'s test was abnormal. Patients were excluded from the study if they had abnormal Allen\'s and modified Allen\'s test, were on haemodialysis and had abnormal serum creatinine level .
Transradial coronary angiography was defined successful on a subjective basis if both the right and left coronary arteries were visualized completely judged by the attending cardiologist. Transradial angioplasty was defined successful when accomplished completely from radial artery approach along with achievement of thrombolysis in myocardial infarction (TIMI) grade 3 flow and less than 20% residual stenosis in the vessel being treated by interventionist . Radial access time was measured from infiltration of lidocaine to introduction of 0.018 inch guide wire. Procedure time was measured from the point of time patient was ready for procedure until procedure is completed. Fluoroscopy time was defined as the total time of fluoroscopy use during the coronary angiography or angioplasty procedure. Complications were considered as significant if there was a large forearm haematoma with haemoglobin drop of 2mg/dl, requirement of blood transfusion because of blood loss at vascular access or surgical intervention because of acute compartment syndrome and forearm ischaemia.
Allen\'s test is a commonly used, valid clinical screening test for assessment of hand circulation and to prevent ischaemic complication of the hand.10 The Allen\'s test was performed by asking the patient to clench the fist for 1 minute while both radial and ulnar arteries were compressed with the examiner\'s fingers. The palm of the hand blanched. Then compression of ulnar artery was released; the normal colour of palm returned within 10 seconds, if there was adequate collateral circulation. A positive test was reported when there was abnormality in the capillary filling of the fingers in 10 seconds. The modified Allen\'s test was performed similarly except radial artery was released instead of ulnar artery and normal blush of hand was noted.
All procedures were performed or supervised by two interventionist with significant experience in transradial interventions. The choice of coronary intervention equipment including guiding catheters, guidewires, angioplasty balloons or stents was on the discretion of the incharge interventionist. All patients had their radial artery checked manually before discharge to identify radial artery occlusion.
A proforma was designed to record patient demographics including age,gender, cardiac risk factors, patient height and weight, total procedure time, radial access time, fluoroscopy time, type of coronary diagnostic catheter and equipment used during PCI and the number of coronary vessels attempted for PCI. Also included in the proforma was mode of intervention (whether primary, rescue angioplasty or elective PCI), failure and success rates of TRCAG and TRCAP along with any associated complications.
The collected data was entered and analyzed by the Statistical Package for Social Sciences version 15.0 Software (SPSS Inc., Chicago, Illinois).
Continuous variables like age (years), height (cm), weight (kg), total procedure time (minutes), radial access time (seconds) and fluoroscopy time (minutes) were presented as Mean ± S.D. and categorical variables such as gender, cardiac risk factors, type of coronary diagnostic and interventional equipment and number of coronary vessels attempted for PCI, success and complications were given as percentages.
Results
A total of 182 (76.3%) coronary angiographies and 82 (76.8%) coronary angioplasties were preformed from the trans-radial route in the study period. The right hand was selected in 263 (99.6%) cases. The 6F sheath was most commonly used in 261 (98.5%) and 7 F sheath was used in 3 (3.6%) cases. Our study population comprised of 199 (75.4%) males and 64 (24.6%) females with mean age of 57 ± 11.08 years (Table-1).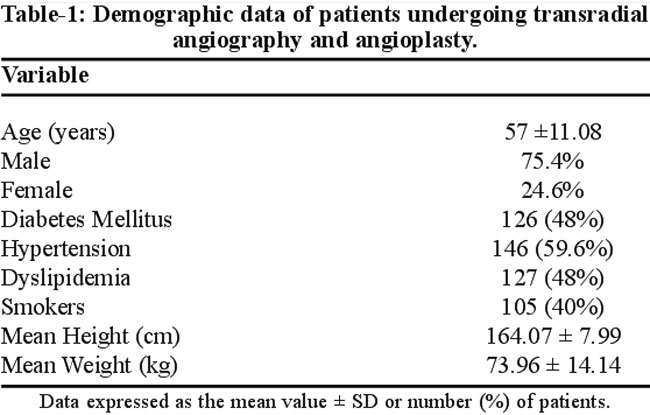
Out of 264 cases, 119 (45%) were elective and 4 (1.5%) had primary PCI. The rest of 141(53%) patients had acute coronary syndrome, post-MI angina, worsening stable angina and assessment of coronary anatomy before valvular surgery (Table-2).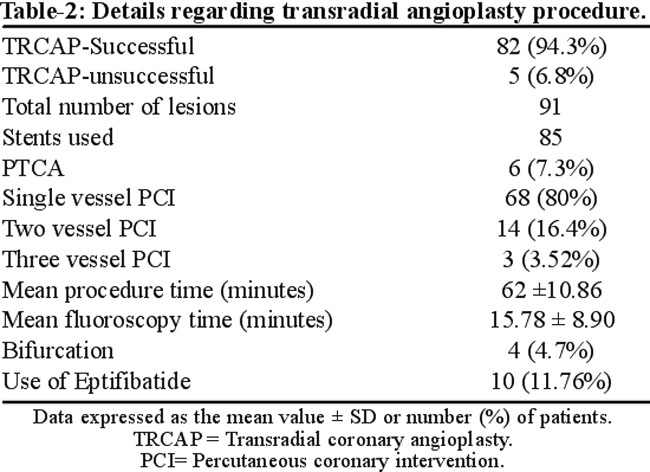
Total of 74 (40%) patients who underwent trans-radial angiography were discharged after 4 hours. The mean radial artery access time was 42.56 ±18.75 seconds. The overall procedural success rate was 182 (90.5%) for TRCAG. The reasons for failure of transradial procedure included failed radial artery puncture (n=4), radial artery loop (n=1), tortuous sub-clavian artery 2 (0.75%), failed catheterization of coronary arteries 4 (1.5%) and severe radial artery spasm 7 (2.65%).The tiger catheter was successful in selective catheterization of both coronary arteries in 164 (90.32%) cases. The mean fluoroscopy time for TRCAG was 5.65 ± 2.3 minutes and the mean procedure time was 23.74 ± 6.26 minutes. TRCAP was attempted in 88 patients with success in 83 (94.3%) and failed in 5 (6.8%) patients. The reasons for failure of TRCAP were radial artery spasm 2(2.4%), tortuous sub-clavian artery 1(1.2%), difficulty engagement of guide and poor guide support 2 (2.4%). A total of 91 lesions were treated, stents were implanted in 85 (93.4%) lesions and plain balloon dilatation was performed in 6 (7.3%).A 6F guiding catheter was used in 80 (98.4%) and 7F guiding catheter was used in 2 (2.4 %). The mean fluoroscopy time for TRCAP was 15.78 ± 8.90 minutes and mean procedure time was 62 ± 10.86 minutes. All procedures from radial artery approach ended up safely with standard anticoagulation. There were no major complications encountered in our study, one patient (0.37%) suffered minor forearm haematoma and was treated conservatively. Asymptomatic radial artery occlusion occurred in 4 (1.5%) study patients.
Discussion
Radial artery approach for coronary intervention has shown to reduce access site complications; early ambulation and reduced hospital stay.7 Unfortunately, radial access still accounts for less than 10% of procedures worldwide.8 Assumption that radial artery approach has excess failure rate and prolonged procedure time could have been the reasons for underutilization of radial artery site.11 More data is required to convince interventional cardiologist to change their practice.
International data has demonstrated that coronary interventions can be performed more safely than contemporary femoral route. Even the most successful coronary percutaneous intervention can be complicated by vascular access site complications in as much as 2-8% of cases performed from transfemoral route.4,12 The ACCESS study clearly demonstrated reduction of major access site complications from radial compared to femoral and brachial approaches (0% vs 2.3% vs 2%% respectively).12 In a recent meta- analysis of 22 randomized controlled trials by Sanjit S Jolly et al,13 radial access reduced major bleeding by 73% compared to femoral access (0.05% vs 2.3%) , OR 0.27 [95% CI 0.16-0.45], p<.001). Reduction in access site complications is really important in current era when more high risk interventions are performed in more sick patients with concomitant use of multiple anti-platelet and anti-coagulant medicines. No major access site complications occurred in radial group compared to 7.5% complications at entry site in femoral group among patients receiving abciximab during percutaneous intervention (PCI).4 Transfemoral intervention in acute myocardial infarction carries a risk of access site complications of up to 23%.14 On the contrary almost no access site complications have been described in patients undergoing transradial PCI in acute myocardial infarction who received GpIIb/IIIa inhibitors.15,16 Our study has also validated that transradial route reduces vascular access site complications considerably, as only one patient (0.37%) developed minor forearm haematoma which settled successfully with conservative treatment.
A study performed at National Institute of Cardiovascular diseases found transradial diagnostic coronary angiogram and percutaneous intervention results to be comparable to femoral approach in terms of success but without any major vascular access site complications.17
The failure to complete the procedure from radial artery approach has been relatively high and related to radial artery spasm, radial loops, subclavian artery tortuosity and dilated aortic root.3 Transradial approach has a learning curve period and the failure rate is especially high during this period. With experience, failure rate could be reduced from 10% to 1 % after 1000 cases.11 The failure to complete the procedure from radial route was 6% for TRCAG and 6.8% for TRCAP in our study. The failure or cross over rate of radial access site was 5.9% in the meta-analysis by Jolly et al,13 compared to 1.4% in the femoral group. A dichotomous trend was noted in cross over or failure rate in the studies performed in the early era of radial access (before 1999) and the recent era (1999-2008). The odds of access site cross over was 5-fold higher in early era and reduced to 3-fold in modern era, suggesting technology and expertise have narrowed the gap.13
Transradial procedures tend to be technically more challenging and time- consuming especially during initial learning curve period.11 The mean procedure time and mean fluoroscopy time for TRCAG was 23.74 ± 6.26 minutes and 5.65 ± 2.3 minutes respectively in the current study. For TRCAP, mean procedure time was 62 ± 10.86 minutes and mean fluoroscopy time was 15.78 ± 8.90 minutes. In the CARAFE study,18 the procedural duration from the radial approach was 12.4 ± 5.8 min and fluoroscopy time was 3.8 ± 2.2 min for coronary angiography. The procedural time in the transradial group (40.2 min) was longer than the transfemoral approach (37.0 min) in the study by Brueck et al,19 but it was recognized that if sheath removal time of transfemoral procedure had been included, the procedure duration would have been similar.19 This has been demonstrated that radial experts have shorter procedure time compared to non-radial experts.13
Asymptomatic radial artery occlusion occurs in 3-5% of patients in different studies.20 Asymptomatic, in hospital radial artery occlusion occurred in 1.4% of our study population. No post discharge follow ups were done, so this number could be an under-estimate. Majority of occluded radials are known to recanalize overtime.21
The limitation of our study was the absence of a comparative femoral group, because of very small volume of transfemoral procedures performed in our catheterization laboratory. Another limitation was lack of follow up for identification of radial artery occlusion or any other complication.
Conclusions
The radial artery approach is found to be very safe with high degree of success and low vascular access site complications for coronary diagnostic and interventional procedures in local population. The beginners of radial approach have to go through a learning curve period patiently, as during this period both procedural failure and long procedure time is expected.
Acknowledgement
We acknowledge the efforts of Dr. Hammad Ali Qazi and Mr. Iqbal Mujtaba for their statistical assistance.
References
1.Moscucci M, Fox KA, Cannon CP, Klein W, López-Sendón J, Montalescot G, et al. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coronary Events (GRACE). Eur Heart J 2003; 24: 1815-23.
2.Campeau L. Percutaneous radial artery approach for coronary angioplasty. Catheter Cardiovasc Diagn 1989; 16: 3-7.
3.Kiemeneij F, Laarman GJ. Percutaneous transradial artery approach for coronary stent implantation. Catheter Cardiovasc Diagn 1993; 30: 173-8.
4.Choussat R, Black A, Bossi I, Fajadet J, Marco J. Vascular complications and clinical outcomes after coronary angioplasty with platelet IIb/IIa receptor blockade. Comparison of transradial vs transfemoral arterial access. Eur Heart J 2000; 21: 662-7.
5.Cruden NL, Teh CH, Starkey IR, Newby DE. Reduced vascular complications and length of stay with transradial rescue angioplasty for acute myocardial infarction. Catheter Cardiovasc Interv 2007; 70: 670-5.
6.Philippe F, Larrazet F, Meziane T, Dibie A. Comparison of transradial versus transfemoral approach in the treatment of acute myocardial infarction with primary angioplasty and abciximab. Catheter Cardiovasc Interv 2004; 61: 67-73.
7.Cooper CJ, El-Shiekh RA, Cohen DJ, Blaesing L, Burket MW, Basu A, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: a randomized comparison. Am Heart J 1999; 138: 430-6.
8.Hamon M, Mehta S, Steg G, Faxon D, Kerkar P, Joyner C, et al. Major bleeding in patients with acute coronary syndrome undergoing early invasive management can be reduced by fondaparinux, even in the context of trans-radial coronary intervention: Insights from OASIS-5 Trial.Circulation 2006; 114: 552.
9.Wu CJ, Lo PH, Chang KC, Fu M, Lau KW, Hung JS. Transradial coronary angiography and angioplasty in Chinese patients. Catheter Cardiovasc Diagn 1997; 40: 159-63.
10.Kohonen M, Teerenhovi O, Terho T, Laurikka J, Tarkka M. Is the Allen test reliable enough? Eur J Cardiothorac Surg 2007; 32: 902-5.
11.Louvard Y, Pezzano M, Scheers L, Koukoui F, Marien C, Benaim R,etal. Coronary angiography by a radial approach: feasibility, learning curve .One operator\'s experience. Arch Mal Coeur Vaiss 1998 ; 91: 209-15.
12.Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T , Vander Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the ACESS study. J Am Coll Cardiol 1997; 29: 1269-75.
13.Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: A systematic review and meta-analysis of randomized trials. Am Heart J 2009; 157: 132-40.
14.Cantor WJ, Kaplan AL , Velianou MH, Barsness GW, Berger PB, Ohman EM. Effectiveness and safety of abciximab after failed thrombolytic therapy. Am J Cardiol 2001; 87: 439-42.
15.Saito S, Tanaka S, Hiroe Y. Comparative study on transradial approach vs transfemoral approach in primary stent implantation for patients with acute myocardial infarction: Results of the test for myocardial infarction by prospective unicenter randomization for access sites (TEMPURA) trial .Catheter Cardiovasc Interv 2003; 59: 26-33.
16.Brasselet C, Tassan S, Nazeyrollas P, Martial Hamon, Damien Metz. Randomized comparison of femoral versus radial approach for percutaneous coronary intervention using abciximab in acute myocardial infarction: results of FARMI trial. Heart 2007; 93: 1556-61.
17.Saghir T, Jan DM, Masood T, Shafi T, Qamar SN, Kundi A. Transradial diagnostic and Percutaneous Intervention . J Coll Physicians Surg Pak, 2003; 13: 242-7.
18.Louvard Y, Lefèvre T, Allain A, Morice M. Coronary angiography through the radial or the femoral approach: The CARAFE study. Catheter Cardiovasc Interv 2001; 52: 181-7.
19.Brueck M, Bandorski D, Kramer W, Wieczorek M, Höltgen R, Tillmanns H. A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. JACC Cardiovasc Interv. 2009; 2: 1047-54.
20.Stella PR, Odekerken D, Kemeneij F, Laarman GJ, Slagboom. Incidence and outcome of radial artery occlusion following transradial coronary angioplasty. Catheter Cardiovasc Diagn 1997; 40: 156-8.
21.Caputo RP, Simons A, Giambartolomei A, Grant W, Fedele K, Abraham S, et al. Safety and efficacy of repeat transradial access for cardiac catheterization procedures. Catheter Cardiovasc Interv 2001; 54: 188-90.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: