
Faisal Azam ( Medical Oncology, Churchill Hospital, Oxford, United Kingdom. )
Mohammad Shams-ul-Islam ( Medical Oncology, Churchill Hospital, Oxford, United Kingdom. )
August 2010, Volume 60, Issue 8
Review Articles
Abstract
Human Papilloma virus (HPV) is present in all the cases of cervical cancer. It can also cause other diseases like genital warts, condylomata accuminata, cervical intraepithelial neoplasia and Anogenital cancers. Cervical cancer is the second most common cause of death from cancer. To improve the mortality from cervical cancers it is extremely important to prevent the HPV infection. In this review we have discussed the role of HPV vaccines in preventing the HPV infections and so the cervical cancer.
Introduction
Infection with human papillomavirus (HPV) is very common in sexually active young adults and adolescents. Approximately 1-2% of sexually active adults worldwide acquire anogenital warts due to HPV every year, with more than 30 million individuals affected yearly.1-3 HPV are classified as high risk for malignancy (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, and 82), probable high risk (26, 53, and 66), and low risk (6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81, and CP6108). Genital warts are the most common sexually transmitted disease, and abnormal cervical cytology or dysplasia are the most common clinical manifestation of HPV infection and cause a big health care burden to patients and health care providers. Cervical cancer was the first malignancy attributed to HPV infection, with HPV detected in more than 99% of cervical carcinomas. HPV 16 and 18 together are found in about 70% of cases.4 Cervical cancer is the second most common cause of death from cancer after breast cancer among women worldwide. Vulvar, vaginal, and penile cancers are also caused by HPV infection.
Majority of men and women infected with HPV do not get clinical disease and host immune system resolve the infection through cell mediated immune response to HPV antigens especially E6 and E7, which play crucial roles in the clearance of transient HPV infections. HPV specific antibody responses are thought to prevent subsequent infections, and antibody production is the primary goal of prophylactic vaccines.
The interval between acquisition of HPV infection and malignant progression takes more than 10 years. Cervical cancer therefore is rare in women under 25 years of age, the incidence rises with the age and is highest in women over 40. Around 80% of cervical cancer occurs in developing countries. One of the main reasons for that is non-existence of cervical screening programmes or testing for the presence of cervical HPV DNA, so HPV vaccination might be the best way to prevent HPV related cancers.
The first prophylactic vaccine for HPV, Gardasil® (Merck and Co) was approved in the United States in 2006, with a second vaccine, Cervarix® (GlaxoSmithKline), which is already in use internationally. Although no therapeutic vaccine has been approved but several different methods of vaccination are currently under investigation. The field of therapeutic HPV vaccination will likely see many more advances in the near future. Decrausaz et-al recently reported 100% tumor protection against subcutaneous TC-1 tumours in mice. CD8 T cells, in those mice that received a single subcutaneous vaccination of an adjuvant long synthetic HPV16 E71-98 polypeptide, mainly provided tumour regression.5 Another study reported significant regression of pappilomas in rabbits following immunization with CRPV (cottontail rabbit papillomavirus) VLPs (virus like particles). This demonstrates the therapeutic potential of pappiloma virus VLPs and its potential for human therapeutic vaccination.6
HPV Pathogenesis:
In order to understand the role of vaccine in prevention of cervical cancer it is essential to understand HPV pathogenesis. Many types of oncogenic HPV are recognised (Table), but HPV16 and HPV18 account for 50% and 20% of cervical cancer respectively.7 These 2 and other types account for other genital and mucosal cancers (Table).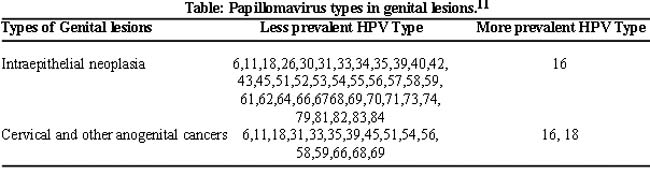
HPV infection requires the availability of epidermal or mucosal epithelial cells that are still proliferating (basal layer cells).
HPV is a DNA virus of 8000 base pairs. The genes encoded by the HPV genome is divided into three regions: an upstream regulatory region that is noncoding and controls transcription of the adjacent open reading frames (ORFs), or coding sequences; the early region, consisting of the E1, E2, E4, E5, E6, and E7 ORFs, which are involved in viral replication and oncogenesis; and a late region, encoding the L1 and L2 viral capsid structural proteins.8 Early (E) and late (L) genes depend on when they are expressed during the HPV life cycle. Currently, 96 HPV types have been identified and fully sequenced; data suggests that almost 200 types exist.9 These viruses show strict cellular tropism, infecting only the epithelial cells of their hosts.
Following entry into the suprabasal layers late viral genes expression starts, which are involved in the assembly of infectious HPV virions during final stages of infection. E5 stimulates cell growth by forming complex with epidermal growth factor receptor; the platelet derived growth factor -receptor and colony stimulating factor-1 receptor. It also prevents apoptosis following DNA damage. Substantial parts of the genome including E5 coding sequence is deleted in late events of HPV mediated carcinogenesis. E6 and E7 genes are consistently expressed in malignant tissues and inhibiting their expression blocks the malignant phenotype of cervical cancer cells. E6 inhibits p53 tumour suppressor genes, while E7 inhibits RB tumour suppressor gene. E1 and E2 are viral regulatory genes. The 2 structural proteins L1 and L2 (Late proteins) are not expressed in precancerous and malignant cells but when expressed in eukaryotic cells, both L1 and L2 are able to self assemble to form virus like particles (VLPs), which cannot be distinguished from mature virions except that they lack viral DNA. L1 is able to self-assemble when expressed independently, whereas L2 is incorporated into VLPs when coexpressed with L1.10 L1 and L2 have been identified as ideal targets for prophylactic vaccination as they are expressed in early infection.
Prevention of Cervical Cancer:
Routine vaccination programmes have had a substantial impact on reducing the prevalence of a variety of diseases. In light of the fact that HPV is a prerequisite for virtually every case of cervical cancer and genital warts occurring worldwide, vaccination may be the most effective mechanism to prevent HPV infection and HPV associated diseases.
Current cervical screening reduces mortality from cervical neoplasia; it does not however, prevent HPV infection or development of pre malignant lesions, such as high-grade cervical intraepithelial neoplasia (CIN 2/3) all of which may require treatment. A vaccine that protects against HPV infection would be expected to reduce the morbidity, mortality and cost burden of HPV associated diseases. Reducing death from cervical and HPV induced cancers is the most important goal of the HPV vaccine.
HPV Vaccines:
HPV vaccine development commercially began in 1993 following a decade and half of intense academic research that proved the link between the HPV and cervical cancer and elucidated the basic natural history of the virus.
In a randomised, multicentre, double blinded, placebo controlled study in young women, monovalent VLP (virus like particles) vaccines was found to be safe, well tolerated and highly immunogenic. Anti-HPV antibody levels were found to be higher than natural infection. It was 100% efficacious in preventing HPV-16 associated cervical dysplasia. Overall 99.7% of women who received the vaccine formulation seroconverted to anti-HPV 16 antibody-positive.12
Trial on bivalent vaccine (cervarix, by Glaxosmithkline, incorporating HPV-16/18 L1) in 15-25 years old, with < 6 male sexual partners and seronegative for HPV 16 and 18, was 100% effective in preventing persistent HPV 16 or 18 infections after 3 injections, on day1, month1 and month 6. Even in women who didn\'t have all the 3 injections it was found effective in preventing HPV infection but less effective than 3 injections.13 It is effective against HPV 16 and 18, and uses L1 protein derived from the baculovirus expression vector in Trichoplusnia cells and has an additional immunogenic adjuvant, AS04.14 AS04 is an immunostimulant monophosphoryl lipid A, which has been shown to induce a greater antibody response than aluminum hydroxide, present as an adjuvant in Gardasil. Although the AS04 adjuvant has been shown to elicit an increased HPVVLP L1 memory B cell response, the clinical significance of this increased response is unclear.15
Trials on quadrivalent vaccine (Gardasil, by Merck, incorporating HPV-16/18/6/11 L1 VLP) in 16-23 years old, with 4 male sexual partners and no history of abnormal pap test, was 100% effective in preventing clinical disease. These women were injected on day 1, month 2 and month 6.16 It uses L1 protein derived from recombinant Saccaromyces cerevisiae.17
The FUTURE-I (Females United to Unilaterally Reduce Endo/Ectocervical Disease) study reported that the quadrivalent vaccine was 100% effective (95% confidence interval (CI) = 94-100) in preventing vaginal, vulvar, perineal, and perianal intraepithelial lesions or warts caused by the vaccine types in the protocol analysis, and 73% (95% CI = 53-83) in the intention-to-treat analysis. The vaccine was also 100% effective (95% CI = 94-100) in the protocol analysis in preventing cervical intraepithelial neoplasia (CIN) grades 1-3 or adenocarcinoma in situ associated with the vaccine types, and 55% effective (95% CI = 40-66) in the intention-to-treat analysis. This was a phase III, randomized, double-blind, placebo-controlled, multinational trial. Quadrivalent vaccine was used in women between the ages of 16 and 24 years and these women were followed over 3 years.18
The FUTURE-II study was a randomized, double blinded, placebo-controlled trial with 3 years of follow-up in 12,167 healthy women aged 15-26, reported that the quadrivalent vaccine is 98% effective (95% CI = 86-100) in preventing any type of high-grade lesion in protocol analysis, and 44% effective (95% CI = 26-58) in the intention-to-treat analysis. A degree of cross protection was seen again, with a 17% efficacy (95% CI = 1-31) in preventing any type of high-grade lesion caused by any HPV type. A subset of the vaccinated women was analyzed in an immunogenicity substudy, which found that 99% of women had seropositivity for the vaccine-type HPVs after vaccination. After 24 months of injection, the per-protocol analysis showed that 96% serpositivity for HPV-6, 97% for HPV-11, 99% for HPV-16 and 68% for HPV 18. This study evaluated the efficacy of the quadrivalent vaccine in the prevention of CIN grade 2 or 3, in situ adenocarcinoma, or invasive cancer.19
The Papilloma Trial against Cancer in Young Adults, a randomized, double-blind, multinational trial that utilized the bivalent vaccine with hepatitis A vaccine as control. An analysis at 15 months after the first vaccine dose reported vaccine efficacy in preventing high-grade lesions caused by HPV types 16 and 18 as 100% (95% CI = 74.2-100). Cross-protection was also seen against persistent infection by HPV 45 (59.9%; 95% CI = 2.6-85.2), 31 (36.1%; 95% CI = 0.5-59.5), and 52 (31.6%; 95% CI = 3.5-51.9), and to a lesser degree, 12 other nonvaccine oncogenic types (27.1%; 95% CI = 0.5-46.8). The immunogenicity subset showed over 99.5% seropositivity for the vaccine HPV types after the third vaccine dose.20
Two phase-II studies studied women five years after vaccination, reported the quadrivalent vaccine to be 95.6% effective (95% CI = 83.3-99.5) in preventing persistent infection, and 100% effective (95% CI = 12.4- 100) in preventing disease (cervical dysplasia or genital warts). Anti-HPV geometric mean titers (GMTs) after 60 months was higher than GMTs observed in the placebo group with a previous history of natural HPV infection, suggesting that vaccine-induced immune responses appear to remain at or above GMTs observed in a natural immune response and subsequent clearing of a HPV infection.21
Clinical trials are currently underway for an octovalent vaccine that confers protection against an additional four oncogenic types.22 In Western blot and enzyme-linked immunosorbent assay (ELISA) testing, both HPV type-specific and type-common, or cross-reactive, epitopes have been identified in a region of L2 that is likely to be expressed on the surface of mature virions. L2 has potential as the basis of a prophylactic HPV vaccine; theoretically, the vaccine would be able to induce cross-neutralizing antibodies to many HPV genotypes and would thus not require the incorporation of type-specific L2 in order to confer broad-spectrum protection.23 An L2-based epitope vaccine is currently in development for early-phase clinical trials.24
A systematic review of all randomized controlled trials of vaccines against HPV compared it with placebo for efficacy, safety, and immunogenicity. Six studies included 47,236 women in the review. Bivalent and quadrivalent HPV vaccines significantly reduced the rate of lesions in the cervix, vulva, vagina, and anogenital region, with efficacy of 93% (95% confidence interval [CI], 87-96) and 62% (95% CI, 27-70), respectively, when compared with the control groups according to intention to treat. More symptoms were found in the bivalent vaccine group (35%; 95% CI, 5-73) when compared with the control groups. In regard to vaccine immunogenicity, there was seroconversion in the group that received the vaccine when compared with the placebo group in the bivalent and quadrivalent vaccines. Prophylactic vaccination can prevent HPV infection in women aged 9 to 26 years not previously infected with the HPV subtypes covered by the vaccines.20
Mechanism of Vaccines:
These vaccines are non-infectious subunit virus like particles (VLP) of a major capsid protein, L1, which is a major structural protein of the virus and closely mimic natural HPV virions. L1 protein has the intrinsic ability to self assemble into VLPs that can induce high levels of neutralizing IgG antibodies. IgG is the principal immunoglobulin in cervical secretions and protection is mediated by serum IgG (neutralising IgG) that can transude across the cervical epithelium particularly at squamo-columnar junction to bind to virus particles and prevent infection.26 Serum IgG level is higher than cervical secretion and it is possible that potential sites of infection on cutaneous and mucosal epithelial surfaces may have access to systemic antibodies. Epithelial microtrauma as occurs during intercourse causes infection and increases exposure to systemic IgG.
There is a role of T cells in clearing HPV infections. Resolution of HPV lesions is accompanied by a CD4 T lymphocyte dependant response. Effective T cell response could add to the efficacy of a prophylactic vaccine by mopping up any infected cells resulting from the virus breaking through antibody defences.
The immunodominant epitopes in L1 VLP induce neutralizing antibodies that are type specific. It has therefore been necessary at least for the first generation HPV vaccines to focus on HPV types found most frequently in cervical cancer, HPV16 & HPV18. Phase 2 and phase 3 trials of these vaccines demonstrate that the patients are protected from cervical HPV induced disease, while the Gardasil also protect against HPV 6/11 induced mucosal and cutaneous genital diseases. Duration of protection is not exactly known but it has been evident from trials that antibody level falls from the peak after immunization to plateau level over 2 years and persist for at least 48 months post vaccination.27,28
Administration Protocol:
Cervarix: 0.5 ml intramuscular injection at 0, 1, 6 months
Gardasil: 0.5 ml intramuscular injection at 0, 2, 6 months
It was thought that prime boost vaccination in non cervical anogenital intraepithelial neoplasia (AGIN) would be beneficial. In one of the non randomised trial women with biopsy proven AGIN were vaccinated with prime vaccination comprising HPV 16, E6/E7/L2 (TA-CIN) on days 0, 28 and 56 followed by one dose of vaccinia virus encoding HPV 16 and 18 E6/E7 (TA-HPV) on day 72. This approach offered no advantage over single TA-HPV vaccination.29
These vaccines are usually safe and very well tolerated but few of the recognised side effects are pyrexia, pain, swelling and erythema at the injection site, pruritis, bronchospasm and urticaria. A pooled analysis of the safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted cervical cancer vaccine Cervarix, performed in a cohort of almost 30,000 girls in 11 trials, reported that the vaccine had a favourable safety profile in women of all ages.30
Indications:
These vaccines should be delivered to young women before exposure to the virus so to prevent high-grade cervical dysplasia (CIN 2/3), cervical carcinoma, high grade vulvar dysplastic lesions (VIN 2/3), and external genital warts (condylomata acuminata). Protective efficacy in men is not known. But For vaccination to have maximum benefit, ideally both men and women should be vaccinated. HPV vaccine may be licensed for men in the near future. Interesting findings of the study on acceptability of HPV vaccine in men reported that informing men about the benefits of male HPV vaccination for reducing cervical cancer risk in women does not increase men\'s interest in the vaccine. This will have important implications for future HPV vaccination campaigns targeting young adult men.31
Problems associated with Vaccination:
Duration of vaccine induced immunity is not known.
Protective responses may involve local antibody levels in cervical secretions; however, none of the efficacy studies have addressed this issue.
Detection of genotype specific HPV capsid antibody in serum correlate with vaccine induced protection. However each laboratory defines a reactive result differently and there is no agreed definition of what level of response indicates sero-reactivity. Standardization of assays for HPV capsid antibody will therefore assist with HPV vaccine development and epidemiology.32
As cervical cancer is more common in developing countries with no screening programmes, vaccination against HPV is ideal in preventing it but these are expensive and probably will not be affordable by most of these countries. In developing countries, cervical cancer tends to affect relatively young poor women and is the single largest cause of years of life lost to cancer. Currently, the prohibitive cost of the vaccine precludes its widespread implementation but cooperation between governments, international health organizations, and the vaccine industry is needed to overcome this significant barrier so that women are no longer denied a potentially life-saving advance. Worldwide HPV vaccination and cervical cancer screening should be made an international priority.33
Compliance with HPV vaccine in adolescents is a problem. It requires at least 3 visits.
For vaccination in this age group parental consent may be needed, which will be a problem for those adolescents who feel uncomfortable to discuss sexual issues with them, so educating parents, health care practitioners especially paediatricians in this regard is very important.
Vaccine acceptance is largely determined by health beliefs, such as the individual\'s perceived susceptibility to the disease, cost, efficacy and obstacles to obtain the vaccine.
Parents, physicians, political and religious leaders may oppose vaccination on moral grounds, believing that such vaccination encourages sexual activity.
Vaccine could have a negative effect on screening, offering false security to vaccinated women, who may incorrectly believe that they no longer need to undergo pap smear.
More education of the disease and vaccination will help to overcome some of those problems. An Internet based study discussed common beliefs of the parents regarding vaccines and considered reliable vaccine information websites and pamphlets addressing common vaccine safety concerns, the most helpful materials to be used during discussions with parents.34
Media can play a crucial role in raising the awareness and educating public regarding cervical cancer, its association with HPV virus and prevention. To determine the knowledge and attitudes towards HPV vaccination, a study was conducted in Birmingham, UK and reported poor knowledge of HPV and its links with cervical cancer among the study population. Around, 81% had a knowledge score of zero. The majority (88%) of participants were in favour of vaccination, with 83.6% indicating that they would allow a child under their care to be vaccinated.35
Prophylactic HPV vaccination has been perceived differently in different cultures. In this regard a qualitative study in Malaysia included 40 women from different ethnic groups. These women reported their concerns that they might be considered as promiscuous and sexually active. There was a concern if it is halal.36 To be successful in prevention one has to take into account social and cultural acceptability. Religious leaders can play a major role in this regard.
Impact of Prophylactic Vaccination:
Data from the longitudinally observed Guanacaste cohort suggest that eradicating HPV 16,18 from the population would result in a 17% overall reduction in Pap abnormalities, with reductions of 8% in ASCUS (atypical squamous cells of undermined significance), 23% in LSIL (low grade squamous intra epithelial lesions), 45% in HSIL (high grade squamous intra epithelial lesions), and 72% in invasive cancer.37 Thus, the greatest impact of vaccination on cytologic diagnosis will be a reduction in HSIL, while impact on atypical and low grade cytology will be less. Since these borderline cytologic changes make up the majority of colposcopy referrals for biopsy, this will be reduced with the wide spread use of vaccination.
A vaccine against HPV 16,18 can decrease cervical cancer risk by up to 70%, only if given before exposure to the virus. The impact on abnormal cytology and cervical intraepithelial neoplasia (CIN) is less but still substantial.
Conclusion
Infection with human papillomavirus (HPV) is very common in sexually active young adults. Abnormal cervical cytology or dysplasia are the most common clinical manifestation and causes a big health care burden to health care providers. It is detected in almost all of the cervical carcinomas. HPV 16 and 18 together are the commonest types. As cervical cancer is the second most common cause of death from cancer after breast cancer among women worldwide, prevention of the HPV infection is considered to be vital in preventing cervical cancer. Cervical screening in developed countries has played a major role in its prevention but introduction of two of the HPV vaccines should help the cause further. As these vaccines have been in practice for only few years, we do not have much knowledge of its safety and efficacy. But recent safety data from experience in 6 countries (U.S.A, U.K, Australia, Germany, France and Canada) has reported HPV vaccines to be safe, effective and of great importance for women\'s health.38 Both vaccines require ongoing and careful monitoring and especially as WHO is recommending their inclusion in national immunization programmes.39
References
1.Tatti S, Swinehart J, Thielert C, Tawfik H, Mescheder A, Beutner K. Sinecatechins, a defined green tea extract, in the treatment of external anogenital warts: a randomized controlled trial. Obstet Gynecol 2008: 111: 1371-9.
2.Ferenczy A, Franco EL. Prophylactic human papillomavirusvaccines: potential for sea change. Expert Rev Vaccines 2007; 6: 511-25.
3.Kjaer S, Tran TN, Sparen P, Tryggvadottir L, Munk C, Dasbach E, et al. The burden of genital warts: a study of nearly 70,000 women from the general female population in the 4 Nordic countries. J Infect Dis 2007; 196: 1447-54.
4.Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummar JA, Shah KV, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999; 189: 12-9.
5.Decrausaz L, Revaz V, Bobst M, Corthésy B, Romero P, Haefliger DN. Induction of human papillomavirus oncogene-specific CD8 T cell effector responses in the genital mucosa of vaccinated mice. Int J Cancer 2009; 126: 2469-78.
6.Govan VA, Rybicki EP, Williamson AL. Therapeutic immunisation of rabbits with cottontail rabbit papillomavirus (CRPV) virus-like particles (VLP) induces regression of established papillomas. Virol J 2008, 20: 5: 45.
7.Munoz N, Bosch FX, Castellsague X, Diaz M, deSanjose S, Hammouda D, et al. Against which human papillomavirus types shall we vaccinate and screen? The International perspective. Int J Cancer 2004; 111: 278-85.
8.Burd E. Human papillomavirus and cervical cancer. Clin Microbiol Rev 2003; 16: 1-17.
9.deVilliers EM, Fauquet C, Broker TR, Bernard HU, zurHausen H. Classification of papillomaviruses. Virology 2004; 324: 17-27.
10.Kirnbauer R, Taub J, Greenstone H, Roden R, Durst M, Gissmann L, et al. Efficient selfassembly of human papillomavirus type 16 L1 and L1-L2 into virus-like particles. J Virol 1993; 67: 6929-36.
11.Hausen HZ. Papilloma viruses and cancer: from basic studies to clinical application. Nature Rev Cancer 2002; 2: 342-50.
12.Koutsky LA, Ault KA, Wheeler CM, Brown DR, Barr E, Alvarez FB, et al. A controlled trial of a human papillomavirus type 16 vaccine. N Engl J Med 2002; 347: 1645-51.
13.Harper DM, Franco EL, Wheeler C, Ferris DG, Jenkins D, Schuind A, et al. Efficacy of bivalent L1 virus like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: a randomised controlled trial. Lancet 2004; 364: 1757-65.
14.Cervarix® package insert. Rixensart, Belgium: GlaxoSmith- Kline Biologicals, 2007.
15.Giannini S, Hanon E, Moris P, Van Mechelen M, Morel S, Dessy F, Fourneau MA, et al. Enhanced humoral and memory B cellular immunity using HPV16/18 L1 VLP vaccine formulated with the MPL/aluminium salt combination (AS04) compared to aluminium salt only. Vaccine 2006; 24: 5937-49.
16.Villa LL, Costa R L, Petta CA, Andrade RP, Ault KA, Giuliano AR, Wheeler CM, et al. Prophylactic quadrivalent human papillomavirus (type 6, 11,16 & 18) L1 virus like particle vaccine in young women: a randomised double blind placebo controlled multicentre phase 2 efficacy trial. Lancet Oncol 2005; 6: 271-8.
17.Gardasil® package insert. Whitehouse Station, NJ:Merck & Co., 2007.
18.Garland S, Hernandez-Avila M, Wheeler C, et al. Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N Engl J Med 2007; 356: 1928-43.
19.Future II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N Engl J Med 2007; 356: 1915-27.
20.Paavonen J, Jenkins D, Bosch F, Naud P, Salmeron J, Wheeler CM, et al. Efficacy of a prophylactic adjuvanted bivalent L1 virus-like-particle vaccine against infection with human papillomavirus types 16 and 18 in young women: an interim analysis of a phase III double-blind, randomised controlled trial. Lancet 2007; 369: 2161-70.
21.Villa L, Costa RL, Petta CA, Andrade RP, Paavonen J, Jversen OE, et al. High sustained efficacy of a prophylactic quadrivalent human papillomavirus types 6/11/16/18 L1 virus-like particle vaccine through 5 years of follow-up. Br J Cancer 2006; 95: 1459-66.
22.Ferenczy A, Franco EL. Prophylactic human papillomavirus vaccines: potential for sea change. Expert Rev Vaccines 2007; 6: 511-25.
23.Roden RB, Yutzy WH, 4th Fallon R, Inglis S, Lowy DR, Schiller JT. Minor capsid protein of human genital papillomaviruses contains subdominant, cross-neutralizing epitopes. Virology 2000; 270: 254-7.
24.Huh WK, Roden RB. The future of vaccines for cervical cancer. Gynecol Oncol 2008; 109: S48-56.
25.Medeiros LR, Rosa DD, da Rosa MI, Bozzetti MC, Zanini RR. Efficacy of human papillomavirus vaccines: a systematic quantitative review. Int J Gynecol Cancer 2009; 19: 1166-76.
26.Nardelli-Haefliger D, Wirthner D, Schiller JT, Lowy DR, Hildesheim A, Panci F, et al. specific antibody levels at the cervix during the menstrual cycle of women vaccinated with human papillomavirus 16 virus like particles. J Natl cancer inst 2003; 95: 1128-37.
27.Mao C, Koutsky LA, Ault KA, Wheeler CM, Brown DR, Wiley DJ, et al. 2006. Efficacy of human papillomavirus 16 vaccine to prevent cervical intraepithelial neoplasia: a randomised controlled trial. Obstet Gynecol 2006; 107: 18-27.
28.Zimet GD, Mays RM, Fortenberry JD, Vaccines against sexually transmitted infections: promise and problems of magic bullets for prevention and control. Sex Transm Dis 2000; 27: 49-52.
29.Fiander AN, Tristram AJ, Davidson EJ, Tomlinson AE, Morn S, Baldwin PJ, et al. Prime-boost vaccination strategy in women with high-grade, non cervical anogenital intraepithelial neoplasia: clinical results from a multicenter phase 2 trial. Int J Gynecol Cancer 2006; 16: 1075-81.
30.Descamps D, Hardt K, Spiessens B, Izurieta P, Verstraenten T, Breuer T, et al. Safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine for cervical cancer prevention: a pooled analysis of 11 clinical trials. Hum Vaccin 2009; 5: 332-40.
31.Gerend M, Barley J. Human papillomavirus vaccine acceptability among young adult men. Sex Transm Dis 2009; 36: 58-62.
32.Ferguson M, Heath A, Johnes S, Pagliusis S, Dillner J; Collaboration Study Participants. Results of first WHO international collaborative study on the standardization of the detection of antibodies to human papillomaviruses. Int J cancer: 2006; 118: 1508-14.
33.Hakim AA, Dinh TA. Worldwide impact of the human papillomavirus vaccine. Curr Treat Options Oncol 2009; 10: 44-53.
34.Smith M J, Woods CR, Marshall GS. Parental vaccine concerns in Kentucky. J Ky Med Assoc 2009; 107: 342-9.
35.Walsh CD, Gera A, Shah M, Sharma A, Powell JE, Wilson S. Public knowledge and attitudes towards Human Papilloma Virus (HPV) vaccination. BMC Public health 2008; 8: 368.
36.Wong L P. Young multiethnic women\'s attitudes toward the HPV vaccine and HPV vaccination. Int J Gynaecol Obstet 2008; 103: 131-5.
37.Schifman M. Integration of human papillomavirus vaccination, cytology, and human papillomavirus testing. Cancer 2007; 111: 145-53.
38.Agorastos T, Chatzigeorgion K, Brotherton J M, Garland S M. Safety of human papillomavirus (HPV) vaccines: a review of the international experience so far. Vaccine 2009; 27: 7270-81.
39.Safety of human papilloma virus vaccines. (Online) 2010 (Cited 2008 May 3). Available from URL: http://www.who.int/vaccine_safety/topics/hpv/en.s
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: