
Masoud Tahmasian ( Sleep Research Center, Department of Psychiatry, Kermanshah University of Medical Sciences, Iran. )
Habibolah Khazaie ( Sleep Research Center, Department of Psychiatry, Kermanshah University of Medical Sciences, Iran. )
Amir Ali Sepehry ( Department of Psychology, University of Victoria, Canada. )
Michael B. Russo ( John A. Burns School of Medicine, University of Hawaii, USA. )
June 2010, Volume 60, Issue 6
Review Articles
Abstract
Background: Behavioural and functional activity monitoring has a long history in sleep research. The term "Actigraphy" refers to methods using computerized wrist-watch-size devices (generally placed on the wrist, but also on the ankle or trunk) to record the movement it undergoes. Collected data are displayed on a computer and analyzed for change in rhythm parameters that in turn provide an estimate on wake-sleep parameters (such as total sleep time, percent of time spent asleep, total wake time, percent of time spent awake and the number of awakenings). Actigraphy provides a useful, cost-effective, non-invasive and portable method for assessing specific sleep disorders. The present review is an amalgam of current knowledge with proposed clinical application and for research of actigraph. Conclusion: Actigraphy cannot stand alone as a diagnostic tool for all clinical groups. Particularly so with those diagnosed with sleep disorders with significant motility or long catatonic periods of wakefulness during sleep.
Introduction
Patterns in human body movements (activity) are of interest for many scientific disciplines. Application of accelerometers using miniature motion sensors to study the macro (gross) and micro- (barely discernible) activities associated with human motion has been termed actigraphy. Advances in accelerometry technology resulted in devices that miniaturize these monitoring systems to the size of a digital wristwatch. Nowadays, the terms actigraph and actigraphy have been widely applied in sleep research. In this review, the term actigraph will refer to the sensor, whereas wrist-mounted actigraphy will refer to the use of the sensor on the wrist platform.
Actigraphy has been broadly used to study sleep/wake patterns for over 25 years. Although polysomnography (PSG) is the gold standard for sleep studies, the advantage of actigraphy over traditional polysomnography lies in its continuous ambulatory recording for a day, to weeks or even longer. Since its conception in 1920s, actigraphy was developed to objectively measure and quantify sleep patterns based on body movements. For example, Szymansky in 1922 constructed a device that was sensitive to the gross body movements of subjects while lying in bed.1 However, the advent of electroencephalograph (EEG) recording along with the development of EEG-based polysomnographic standards for the scoring of sleep stages resulted in a shift, distancing this approach from movement-based measurements of sleep.2
A resurgence of interest in the use of movement-based measurement of sleep occurred when wrist-mounted accelerometry was developed in the 1970s and 1980s at the Walter Reed Army Institute of Research (AIR) and the National Institutes of Health (NIH). Wrist-mounted accelerometers were based on technological advances that, for the first time, made long-term portable measurement and recording of movement data feasible.3
In 1995, Sadeh and colleagues under the auspices of the American Sleep Disorders Association (now called the American Academy of Sleep Medicine, AASM), reviewed the literature pertaining to the role of actigraphy in the evaluation of sleep disorders. They concluded that actigraphy provided useful information and that it may be a "cost-effective method for assessing specific sleep disorders but methodological issues have not been systematically addressed in clinical research and practice".4 Based on that task force\'s report, the AASM Standards of Practice Committee in 1995 concluded that actigraphy was not indicated for routine diagnosis or for assessment of severity or management of sleep disorders, but might be a useful adjunct approach for diagnosing insomnia, circadian rhythm disorders or excessive sleepiness.5
Nowadays, wrist-mounted actigraphs have movement detectors and sufficient memory to record for up to several weeks. Analysing programmes are to derive levels of activity/inactivity, rhythm parameters and sleep/wake parameters.6 In addition, PubMed - a service provided by the US national library of Medicine and NIH - shows over 913 citations using actigraphy or actigraph with human subjects, of which 677 are investigating adult individuals (age 19 and over), of which 8 are reviews. Since new devices, sleep-wake scoring algorithms, and operating procedures are constantly developed and up-dated, in this review, we have chosen to elide discussing technical merits of the various instruments, modes of operations, and specific brand names. Furthermore, we position this paper in the light that no consensus of opinion has been reached among clinicians and researchers as to which device or algorithm is best. Additionally, we encourage new users to read the erudite literature on each instrument carefully in order to reach an educated decision as to which combination of device, mode of operation and scoring algorithm is most suitable for a specific research protocol.
Mechanism, data abnormalities, particularities, and conditions:
As summarized elsewhere, we invite readers to familiarize themselves with instrumentation and methods on how to use a miniaturized actigraph to observe and to amass data generated by body motion.6 Highlighting some of the strengths of actigraphy, the proportional integration method was found to be superior to other methods in activity counting by identifying movement amplitude.7 However, discrepancies exist in the literature in reporting data sets from several devices with different data collection strategies and different scoring algorithms.6 Although assessments of placement differences have indicated that scoring algorithms are somewhat insensitive to wrist placement (dominant versus non-dominant hand) in spite of significant differences in activity levels,8 dominant wrist placement was superior to that of all other placements at detecting wakefulness.9 Additionally, in a number of studies, the wrist-mounted actigraph has been placed on the non-dominant wrist, or on the ankle or trunk. Along these lines, the right wrist recorded more activity than the left wrist equally at early and late in the sleeping period, except no differences were found between ankle placements.10 Diverse approaches in monitoring sleep rhythm produces very variable counts for the identical activity, which renders the comparison difficult and contentious. This last point is in concordance with what Jean-Louis and colleagues suggest in a 2001 published study on sleep detection with accelerometer actigraph. Even though relative changes in activity can be meaningful, more direct comparisons following computer processing of the data are inviting and more meaningful (Figure-1).
Artefacts (e.g., from non-compliance of the patients with the suggested method) and potential loss of data during implementation of this technique are some of the issues that have to be taken into account during monitoring,6 since Acebo and colleagues in 1999 a study published in the journal Sleep suggest that about 28% of the collected data are either insufficient for analysis or misleading. Some of these artefacts could be ruled out if the patient is cooperative for instance by keeping logs of sleep time (at bedtime and rise times). Proper use of this log with additional question and answer between the patient and the practitioner is prominent in minimizing the occurrence of any artefacts. Additional concerns lays in how the device can be protected from breakage or loss of calibration, thus it is imperative for a long-term use of actigraph to plan and follow the procedures for examining batteries and preserving equipment.
Actigraphy pros, cons, and etcetera:
Here we present several supporting points and pitfalls of the use of actigraphy; in which advantages tend to compensate for the shortcomings (Table-1).
Additionally, other points have been raised that, based on a given research hypothesis, could fall under either an advantage or a limitation to actigraphy usage. The following list pertains to these points:
a) No "first night" effect in healthy adults with home monitoring of sleep by actigraphy11
b) Actigraphy results are similar to sleep log data on sleep timing, sleep duration, sleep onset and sleep offset12
c) Nurses\' observations of sleep in psychiatric patients were similar to actigraph13
d) When compared to self report, actigraphy can be considered expensive
e) It is expected that the objective and unbiased nature of data produced by the actigraph necessarily would be more accurate than those yielded by subjective assessment techniques such as sleep logs6
Furthermore, actigraphy is used for the assessment of individuals of all ages; examining various sleep disorders such as insomnia,14 disorder owing to breathing difficulties (e.g., asthma, sleep apnoea),15 restless leg syndrome,16 circadian rhythm abnormalities (e.g., sleep schedule disorder,17 jet lag/shift work,18 and other disorders or syndromes (e.g., foetal familial insomnia,16 non 24-hour sleep-wake syndrome19 and REM sleep behaviour disorder.20
I- Disorders in result of mal-respiration:
Although wrist-mounted actigraph measures appear to reflect variations in sleep due to breathing-related disturbances, it is not recommended for this proposes.4 Studies have provided additional information indicating that fragmented sleep or more activity during sleep is associated with breathing disorders using actigraph. Subsequently they concluded, however, that actigraphy is insufficient to identify reliably individuals who suffer from sleep apnoea.15 However, they warrant further studies comparing groups of subjects. Additionally, Sadeh and coworkers in a 1998 published study on sleep and pulmonary function documented increased activity levels and reduced the motionless sleep percentage in a group of non-symptomatic asthmatic children compared with controls. They concluded that sleep fragmentation as seen by actigraph was associated with reduced pulmonary function as measured by peak flow meter.
II- Periodic leg movements (PLMs):
An exciting utility of actigraphy would be in identification of periodic leg movements\' disorder. A full examination of this approach provided strong support that a special actigraph placed on the foot, along with tailored scoring algorithms could provide consistent measures of PLMs.21 To this date, only one-study reports of a high correlation (0.91) between actigraphically scored and PSG scored PLMs. In contrast, the authors of the study concluded that a general index of restlessness is not sufficient to obtain either a reliable estimate of PLMs or a useful algorithm. Subsequent studies used this method to demonstrate positive therapeutic effects of medication - levodopa - for restless leg syndrome.22 Although a relatively high correlation (0.78) was found between the two methods, a recent study however, questions its validity for measuring leg movements and points to the failure of actigraphy by underestimating leg electromyographic activity.19 Additionally, upon the night-to-night error estimates the authors concluded that despite the discrepancy actigraphy could be used to obtain follow-up measures in intervention studies.23
III (i)- Sleep-wake-schedule disorders and syndrome:
The validity of actigraphy in the assessment of sleep disorder such as in insomnolance has been investigated in numerous publications.14 Among which, Wicklow and Espie investigated cognitive components of insomnia with an emphasis on the role of intrusive thoughts in sleep-onset insomnia. The outcome of the last study was a strong predictor of actigraphy as a reliable tool to assess sleep latency by examining the number of intrusive thoughts prior to sleep.
Despite the fact that actigraphy procedures for appraisal and treatment of sleep-schedule disorders have not been systematically recognized, wrist-mounted actigraphy has been accepted as a practical method for assessing sleep in individuals suffering from such disorders.4 In the same vein, in recent years wrist-mounted actigraphy has been used in intervention studies assessing the phase-shifting effects of melatonin in normal individuals24 and in individuals suffering from sleep-phase delay syndrome.17
Wrist-mounted actigraphy for assessing jet-lag and shift work related phenomena has been demonstrated as useful with promising results to detect transient disturbances. For example, in one study, Zopiclone administration after a west-ward flight led to increased sleep duration and sleep consolidation in comparison with Placebo.18
III (ii)- Circadian rhythms and actigraphy:
Activity is a benchmark of circadian rhythms studies of nonhuman primates, and now wrist-mounted actigraphy is operated effectively in a large range of human circadian rhythms investigations.6 Wrist activity emerges as a suitable indicator of entrained PSG sleep phase, and a strong link to entrained endogenous circadian phase. In non-entrained conditions, wrist activity rhythms may shift from the endogenous rhythm of the suprachiasmatic pacemaker; actigraphy still appears to be practical for recognizing distressed sleep because of alterations in circadian rhythms. It is noteworthy to mention that treatments that improve rhythms also improve sleep. There exists evidence that the circadian phase of wrist activity co-varies with the phase of melatonin secretion in delayed sleep phase syndrome (DSPS), supporting the use of actigraphy in helping to diagnose this condition. A variety of methods for analyzing the circadian characteristics of activity data have proved promising; for this reason, additional and formal comparison of these would be useful towards standardizing this method.
Clinical Intervention:
Because actigraphy is a non-invasive technique and allows for objective assessment of sleep for extended periods, it has become a very useful tool for intervention studies. Recent actigraphic studies documented improvement of sleep following administration of both pharmaceutical16 and physiological agents (e.g., light exposure), and behavioural interventions.4 However, studies failed to document changes in sleep following various interventions,25 but one study demonstrated the impact of caffeine consumption on actigraphic sleep measures.26
The advantages of wrist-mounted actigraphy for intervention research are quite evident. The ability to monitor sleep for extended periods provides researchers with high statistical power. Additionally, a growing number of studies support the sensitivity of actigraphy measures used repeatedly during intervention studies. However, those designing studies of patients with specific neurological conditions with co-morbid motor system impairment need to remember that the ultimate measure from actigraphy is the body\'s movement. Evident change in actigraphy measures may be a function of changes in motor behaviour rather than sleep or wakefulness.
Actigraphy and Psychiatric Studies:
Actigraphy has been used to investigate movement and sleep disturbance in psychiatric patients. For instance, Dursun and colleagues conducted a descriptive study of wrist-mounted actigraphy estimation of sleep in Risperidone medicated outpatients suffering from schizophrenia versus those on first-generation antipsychotics, and controls.27 They found a greater degree of night-time associated wrist movement (i.e., higher movement index) in patients on a first generation antipsychotic compared to those on Risperidone (second-generation antipsychotic). Furthermore, Friedman et al. compared wrist actigraphy data with measures of behavioural problems in a sample of patients with Alzheimer\'s disease (AD) who were participating in a larger longitudinal study.28 They found that greater behavioural disturbance was correlated with lower actigraphically estimated sleep efficiency (r = -.35; p<.05) and greater wake after sleep onset (r = .43; p<.01). In a 1999 published study on motor activity and perception of sleep in depressed patients Lemke and colleagues29 demonstrated the use of wrist actigraphy to estimate mean activity levels in psychiatric unit in-patients with major depressive disorder. They found that subjects whose Pittsburgh Sleep Quality Index indicated poor sleep had greater mean nighttime motor activity levels than those who reported good sleep. In addition, subjects with fewer depressive symptoms had lower mean nighttime motor activity levels than those with greater depressive symptoms.
Actigraphy, sleep, and neurocognitive function:
No review has been published in the past decade and only a handful of studies have emerged in PubMed since 2004 investigating the impact of sleep altercation (without the use of psycho-stimulants) on cognitive performance of non-medicated individuals using actigraphic recording as an objective measurement tool. Here we review research evidence published in past recent years, which investigates the direct impact of sleep cycle changes and neurocognitive performance.
Yaffe and colleagues30 in a recent study showed an association between longitudinal cognitive decline and an increased risk of sleep trouble in older, pre-clinical, non-demented, community-dwelling women. Cognitive data was collected using modified Mini-Mental State Examination and Trails B andsleep disturbance records were gathered via actigraphy (Sleepwatch-O, Ambulatory Monitoring, Inc., Ardsley, NY) measuring total sleep hours, sleep efficiency, sleep latency, napping, and time awake after sleep onset. The authors found that cognitive decliners were more liable than non-decliners to experience sleep disturbance at follow-up (13 to 15 years) on most measures. Noteworthy to mention is that women with lower Trails B performance displayed an added likelihood to nap for more than two hours per day (aOR: 1.73; 95% CI: 1.28, 2.33) and cognitive decline on either test was not associated with total sleep time. In the same vein, Desai and working group31 report on the impact of two possible influential neurobehavioural functioning factors, sleep deprivation and the time of day in individuals suffering from mild Obstructive Sleep Apnoea (OSA) and without OSA. Neurobehavioural Assessment Battery - standardized and validated battery was used to examine neuropsychological functioning, and actigraphy was used as a baseline assessment tool for sleep deprivation. The authors concluded that sleep deprivation resulted in poorer neurobehavioural performance for most outcome measures, and in one reaction time task, greater impairment was observed. Additionally, they suggest that individuals with mild OSA are not dissimilar from subjects without OSA in their neurobehavioural reaction to sleep deprivation.
Another study used actigraphy as an indicator to investigate psychophysiological insomnia and its correlate with selective attention. Marchetti and colleagues,32 on the other hand reported that cognitive models of insomnia suggest selective attention may be involved in maintaining the disorder and its assessment is easier via usage of wrist actigraphy. In addition, others using actigraphy investigated the consequences of morning or evening activity on neuropsychological performance in concurrence with sleep quality in older adults. Additionally, Benloucif and colleagues33 found that short-term exposure to either morning or evening structured social (game playing) and physical activity (stretching, low-impact aerobics) significantly improves objective measures of neuropsychological performance and subjective sleep quality in the community-dwelling elderly. Nevertheless, objective measures of sleep did not ameliorate when assessed by actigraphy.
In summary, the literature is scarce and its interpretation is difficult and must be done with caution. Nevertheless, this area of research requires further exploration particularly using validated and standardized neuropsychological batteries in concurrence with different types of actigraphic devices.
Recent Applications:
Use of wake-sleep information has been applied to facilitate the development of mathematical models that aim to predict aspects of cognitive performance. However, wrist-mounted actigraphy potentially has many more applications to cognitive and physical assessment beyond sleep-wake discrimination. For example, studies using advanced techniques reveal that accelerometric sensors can discriminate heart rate, breathing, and life cessation (death) via wrist-mounted actigraphy. For instance, Russo et al. showed physiologic microvibrations identified by digital signal processing techniques, and how these signals appear to be both a life signs indicator and a potentially quantifiable measure of pain (Figure-2 ).34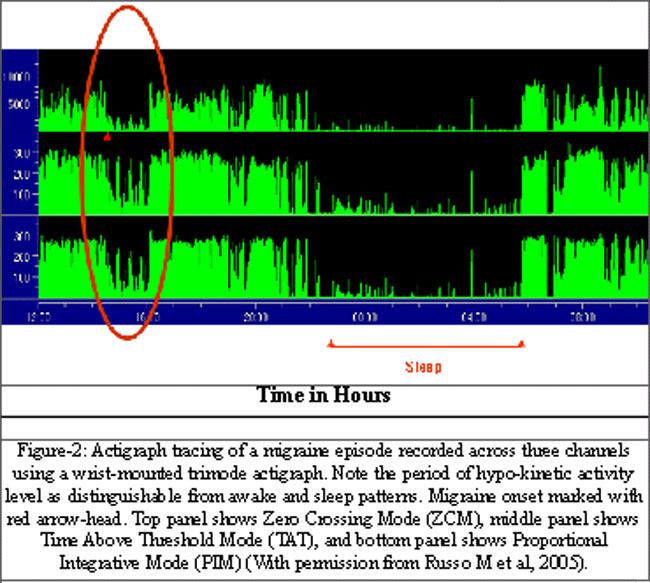
Respirations and heart rate were identified in the actigraphy signal, and removal of cardiac pulsations dramatically reduced the life-signs signal. Death resulted in the cessation of biovibrations (Figure-3).
There is an added potential for wrist-mounted actigraphy in the assessment of cognition through improvements in sleep-scoring algorithms and through increased understanding of the effects of the environment, daily activity, and neurobehavioural functioning on cognitive performance. Wrist-mounted actigraphs can now incorporate environmental cues, such as light levels, ambient temperature and humidity, and ambient noise levels. Interactive devices also may provide a tactile stimulus to which the wearer responds (Figure-4),
enabling measures of alertness and reaction time.35,36
Actigraphy is a tool that records motion signals both physiological and mechanical in origin, but the meaning of the actigraph signal is not self-evident from the signal output. Wrist-mounted actigraphy as a technology is mature and easily applied, but continued research is required to analyze the motion signals and develop the real-time monitoring algorithms necessary to distinguish relevant physiological signals from mechanical components. Applications and validation in operational environments are understudied with little ongoing research to answer even the most basic questions of how to demodulate complex physiological signals.33
The wrist-mounted advanced Digital Signal Processing (DSP) actigraph (PCD, Inc. Fort Walton Beach, Florida) allows recording and characterization of patterns and individual movements, without destroying the information contained within them. Such features as duration, wave shape, amplitude, and component frequencies may be used to describe movements as they occur. These features may be saved and analyzed in relation to sleep, fatigue, exposure to neuro-motor toxins, or specific environmental conditions. The advances in technology permit the application of wrist-mounted actigraphy to identification of subtle physiological motor signals, thereby extending actigraph utility. Additionally, Russo and colleagues in a 2006 study investigating digital signal processing of actigraphy suggest that as uses of wrist-mounted actigraphy continue to expand beyond wake-sleep determinations, DSP actigraphy will most likely play an increasingly prominent role in clinical and operational settings.
Discussion
In summary, although the knowledge to date suggests that actigraphy is not as accurate as PSG for determining sleep state transitions, there is a general agreement that actigraphy, with its ability to record continuously for long periods, is more reliable than sleep logs which rely on the patients\' recall, and is more reliable than observations which capture only short time periods.
Although the 1995 AASM practice parameters paper determined that actigraphy was not appropriate for the diagnosis of sleep disorders, recent studies point to a shift in that for some disorders, actigraphy may be more practical than PSG and can provide information obtainable in no other practical way. While the utility of actigraphy remains controversial in light of diagnosis of sleep disordered breathing or of periodic limb movements, it is highly appropriate for examining the sleep variability (i.e., night-to-night variability) of patients with insomnia. Actigraphy is also appropriate for the assessment of treatment effects of such therapies as hypnotic drugs, light treatment, and CPAP - particularly if assessments have begun prior to the start of treatment. A recent independent review by Sadeh and Acebo reached many of these same conclusions.23
Some of the research studies failed to find relationships between sleep measures and health-related symptoms. The interpretation of these data is ambiguous. For instance, is it that the actigraph is not reliable, which jeopardizes assessing the relationship between sleep changes and quality of life measures; or, is it that, in fact, there is no relationship between sleep patterns and quality of life measures in that population? Additionally, several studies of sleep disorder owing to breathing difficulties fail to find any relationship with quality of life in the absence of actigraphy usage either as an outcome measure or as a screening tool, which encourages us to question the underlying reasons: is it the reliability in actigraphy method, or simply the absence of overall association?
The one area where actigraphy can reliably be applied is in the evaluation of circadian rhythm disorders. Actigraphy has been shown to be a valuable asset in identifying change in the rhythms. Results of actigraphic recordings correlate well with measurements of melatonin and of core body temperature rhythms. Activity records also show sleep disturbance when sleep is attempted at an unfavourable phase of the circadian cycle. Actigraphy therefore would be particularly useful for facilitating the diagnosis of delayed or advanced sleep phase syndrome, non-24-hour-sleep syndrome and in the evaluation of sleep disturbances in shift workers. It is of note that overt rest-activity rhythms are susceptible to various masking effects, so they may not always show the underlying rhythm of the endogenous circadian pacemaker.
On the other hand, actigraphy has a number of limitations. For example, actigraphy cannot detect sleep quality and stages. Potential users should be aware of the pitfalls of actigraphy: (A) validity has not been established for all scoring algorithms or devices, and for all clinical groups; (B) actigraphy is not sufficient for diagnosis of sleep disorders in individuals with motor disorders or high motility during sleep; (C) the use of computer scoring algorithms without controlling for potential artefacts can lead to inaccurate and misleading results.23
In conclusion, the latest set of research studies suggest that in the clinical setting, actigraphy is reliable for evaluating sleep patterns in patients with insomnia; for studying the effect of treatments designed to improve sleep; for diagnosing circadian rhythm disorders (including shift work); and in evaluating sleep in individuals who are less likely to tolerate PSG, such as infants, and the elderly suffering from dementia-type conditions. While actigraphy has been used for research purpose for many years, up to now, methodological issues had not been systematically addressed in clinical research and practice. Those issues have now been addressed, and wrist-mounted actigraphy may now be reaching the maturity needed for application in the clinical arena.
Acknowledgement
This work was supported by Ambulatory Monitoring, Inc (Ardsley, New York), and we wish to thank them for their technical assistance, and lending of actigraph equipments. In addition, we wish to thank Drs. Avi Sadeh (PhD) and Sonia Ancoli (PhD) for their assistance with preparation of this manuscript. The views expressed in this paper represent those of the authors, and not necessarily those of their governments.
References
1.Szymansky J. Aktivitaet und ruhe bei den menschen. Z Angew Psychol 1922; 20: 192-222.
2.Dement W, Kleitman N. Cyclic variations in EEG during sleep and their relation to eye movements, body motility, and dreaming. Electroencephalogr Clinical Neurophysiol 1957; 9: 673-90.
3.Redmond DP, Hegge F. Observations on the design and specifications of a wrist-worn human activity monitoring system. Behav Res Methods Instrum Comput 1985; 17: 659-69.
4.Sadeh A, Hauri PJ, Kripke DF, Lavie P. The role of actigraphy in the evaluation of sleep disorders. Sleep 1995; 18: 288-302.
5.No author listed. Parameters for the use of actigraphy in the clinical assessment of sleep disorders. Sleep 1995; 18: 285-7.
6.Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep 2003; 26: 342-92.
7.Jean-Louis G, Kripke DF, Mason WJ, Elliott JA, Youngstedt SD. Sleep estimation from wrist movement quantified by different actigraphic modalities. J Neurosci Methods 2001; 105: 185-91.
8.Middelkoop HA, van Dam EM, Smilde-van den Doel DA, Van Dijk G. 45-hour continuous quintuple-site actimetry: relations between trunk and limb movements and effects of circadian sleep-wake rhythmicity. Psychophysiology 1997; 34: 199-203.
9.Middelkoop HA, van Dam EM, Smilde-van den Doel DA, Van Dijk G. 45-hour multiple-site actimetry in 20 healthy subjects: relations between body and limb movements and the effects of circadian sleep-wakefulness. Sleep-Wake Research Netherlands 1995: 681-4.
10.Violani C, Testa P, Casagrande M. Actigraphic motor asymmetries during sleep. Sleep 1998; 21: 472-6.
11.Jean-Louis G, von Gizycki H, Zizi F, Spielman A, Hauri P, Taub H. The actigraph data analysis software: I. A novel approach to scoring and interpreting sleep-wake activity. Percept Mot Skills 1997; 85: 207-16.
12.Lockley SW, Skene DJ, Arendt J. Comparison between subjective and actigraphic measurement of sleep and sleep rhythms. J Sleep Res 1999; 8: 175-83.
13.Krahn LE, Lin SC, Wisbey J, Rummans TA, O\'Connor MK. Assessing sleep in psychiatric inpatients: nurse and patient reports versus wrist actigraphy. Ann Clin Psychiatry 1997; 9: 203-10.
14.Natale V, Plazzi G, Martoni M. Actigraphy in the assessment of insomnia: a quantitative approach. Sleep 2009; 32: 767-71.
15.Middelkoop HA, Knuistingh Neven A, van Hilten JJ, Ruwhof CW, Kamphuisen HA. Wrist actigraphic assessment of sleep in 116 community based subjects suspected of obstructive sleep apnoea syndrome. Thorax 1995; 50: 284-9.
16.Benes H, Kurella B, Kummer J, Kazenwadel J, Selzer R, Kohnen R. Rapid onset of action of levodopa in restless legs syndrome: a double-blind, randomized, multicenter, crossover trial. Sleep 1999; 22: 1073-81.
17.Okawa M, Uchiyama M, Ozaki S, Shibui K, Kamei Y, Hayakawa T, et al. Melatonin treatment for circadian rhythm sleep disorders. Psychiat Clin Neurosci 1998; 52: 259-60.
18.Daurat A, Benoit O, Buguet A. Effects of zopiclone on the rest/activity rhythm after a westward flight across five time zones. Psychopharmacology 2000; 149: 241-5.
19.Sforza E, Zamagni M, Petiav C, Krieger J. Actigraphy and leg movements during sleep: a validation study. J Clin Neurophysiol 1999; 16: 154-60.
20.Middleton B, Arendt J, Stone BM. Complex effects of melatonin on human circadian rhythms in constant dim light. J Biol Rhythms 1997; 12: 467-77.
21.Kazenwadel J, Pollmacher T, Trenkwalder C, Oertel WH, Kohnen R, Kunzel M, et al. New actigraphic assessment method for periodic leg movements (PLM). Sleep 1995; 18: 689-97.
22.Karacan I, Williams RL, Littell RC, Sails PJ. Insomnias: Unpredictable and Idiosyncratic Sleeprs. In: Koella WP, Levin P, editors. Sleep: Physiology, Biochemistry, Pharmacology, Clinical Implications. Basel, Switzerland: Karger 1972; 120-32.
23.Sadeh A, Acebo C. The role of actigraphy in sleep medicine. Sleep Med Rev 2002; 6: 113-24.
24.Sadeh A, Raviv A, Gruber R. Sleep patterns and sleep disruptions in school-age children. Dev Psychol 2000; 36: 291-301.
25.Vercoulen JH, Swanink CM, Zitman FG, Vreden SG, Hoofs MP, Fennis JF, et al. Randomised, double-blind, placebo-controlled study of fluoxetine in chronic fatigue syndrome. Lancet 1996; 347: 858-61.
26.Hindmarch I, Rigney U, Stanley N, Quinlan P, Rycroft J, Lane J. A naturalistic investigation of the effects of day-long consumption of tea, coffee and water on alertness, sleep onset and sleep quality. Psychopharmacol 2000; 149: 203-16.
27.Dursun SM, Patel JK, Burke JG, Reveley MA. Effects of typical antipsychotic drugs and risperidone on the quality of sleep in patients with schizophrenia: a pilot study. J Psychiatry Neurosci 1999; 24: 333-7.
28.Friedman L, Kraemer HC, Zarcone V, Sage S, Wicks D, Bliwise DL, et al. Disruptive behavior and actigraphic measures in home-dwelling patients with Alzheimer\'s disease: preliminary report. J Geriat Psychiat Neurol 1997; 10: 58-62.
29.Lemke MR, Koethe N, Shleidt M. Timing of movements in depressed patients and healthy controls. J Affect Disord 1999; 56: 209-14.
30.Yaffe K, Blackwell T, Barnes DE, Ancoli-Israel S, Stone KL. Study of Osteoporotic Fractures Group. Preclinical cognitive decline and subsequent sleep disturbance in older women. Neurology 2007; 69: 237-42.
31.Desai AV, Marks GB, Jankelson D, Grunstein RR. Do sleep deprivation and time of day interact with mild obstructive sleep apnea to worsen performance and neurobehavioral function? J Clin Sleep Med 2006; 2: 63-70.
32.Marchetti LM, Biello SM, Broomfield NM, Macmahon KM, Espie CA. Who is pre-occupied with sleep? A comparison of attention bias in people with psychophysiological insomnia, delayed sleep phase syndrome and good sleepers using the induced change blindness paradigm. J Sleep Res 2006; 15: 212-21.
33.Benloucif S, Orbeta L, Ortiz R, Janssen I, Finkel SI, Bleiberg J, et al. Morning or evening activity improves neuropsychological performance and subjective sleep quality in older adults. Sleep 2004; 27: 1542-51.
34.Russo Vo MB, Labutta A, Black R, Campbell I, Greene WJ, et al. Human Biovibrations: Assessment of Human Life Signs, Motor Activity, and Cognitive Performance Using Wrist-Mounted Actigraphy. Aviation space and environmental medicine 2005; 76: C64-74.
35.Anderson B, Storfer-Isser A, Taylor HG, Rosen CL, Redline S. Associations of executive function with sleepiness and sleep duration in adolescents. Paediatrics 2009; 123: e701-7.
36.Eggermont LH, Knol DL, Hol EM, Swaab DF, Scherder EJ. Hand motor activity, cognition, mood, and the rest-activity rhythm in dementia: a clustered RCT. Behav Brain Res 2009; 196: 271-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: