
Muhammad Tariq Farman ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
Jawaid Akbar Sial ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
Tahir Saghir ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
Syed Nadeem Hasan Rizvi ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
Syed Ishtiaq Rasool ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
Syed Zahid Jamal ( National Institute of Cardiovascular Diseases (NICVD), Karachi. )
February 2010, Volume 60, Issue 2
Case Series
Abstract
Stent dislodgement is a very rare but recognized and potentially serious complication of percutaneous coronary intervention (PCI). This case series describe the incidence and etiology of such cases at National Institute of Cardiovascular Diseases, Karachi during the year 2008 and the method of treatment of this complication
Discussion
Although majority of currently used stents are factory-mounted systems, the risk of stent embolization has not been completely eliminated. Stent dislodgement from the delivery system most often occurs when the stent-balloon assembly is pulled back into the guiding catheter, or when the target lesion cannot be reached or cannot be passed due to unfavorable anatomy.9,10 Stent dislodgement from the balloon was more frequent when stents were manually crimped onto the balloon.
In our first case we wanted to place the stent exactly at the ostium of LAD by using szabo's technique.7,8 Unfortunately we could not properly crimp the stent, therefore, it was dislodged and we could not get the benefit of this technique. Although, it was an obligation to deal with a dislodged stent and we had to crush it against the vessel wall, the technique of crushing a dislodgeded stent is comparatively easier and faster than a number of tedious stent retrieval techniques. It could be used safely and effectively in preference to a number of challenging and sometimes distressing stent retrieval techniques. Of note, every attempt should be made to ensure that the guidewire is outside of the stent to be crushed; otherwise, the wire will be entrapped. Before attempting to crush the stent, passing a balloon distal to a stent ad withdrawing the partially inflated balloon indicates that the wire has not passed through a stent strut, and the technique can then safely be employed.
In the second case, heavy calcification was a hurdle in preparing the vessel for stenting. Despite graduated predilation with two balloons the vessel was still unprepared for stenting and instead of trying forceful placement we should have tried to predilate it with a bigger size balloon. Lesions that cannot be dilated with conventional balloon catheters due to lesion rigidity may also be dilated with Cutting Balloon Angioplasty (CBA),11 and Rotational Atherectomy.12 However, one should not try to stent the poorly prepared artery. Luckily, the stent was not dislodged around the coronary system and as soon as we observed the demounted stent we readily dragged it near the femoral artery where it would not cause much harm to the patient even with embolization.
In the third case the artery was thrombus laden and infarct related and after clot retrieval TIMI-III flow was achieved and apparently it seemed that direct stenting could be done. Secondly, we wanted to avoid distal embolization of residual clot with ballooning. However, this speculation proved incorrect and ended up with dislodgement of the stent although it was retrieved successfully.
Different other percutaneous retrieval techniques have also been described to retrieve embolized stents from the coronary system and the peripheral circulation, including low-profile angioplasty balloon catheters, gooseneck snares, myocardial biopsy forceps, and multipurpose baskets.3,11,12 Compressing the stent against the vessel wall with another stent like we had done in our first case and emergency coronary bypass surgery is considered lesser of the options. In a review by Eggebrecht et al.3 manual crimping of the stent was associated with a significantly higher rate of dislodgement compared to factory-mounted stents and in all cases during retraction of the balloon-stent assembly into the guiding catheter due to failure to reach the lesion site. A low-profile balloon-catheter was the method of choice for retrieving embolized stents, with a high success rate.
References
1.Cishek MB, Laslett L, Gershony G. Balloon catheter retrieval of dislodged coronary artery stents: A novel technique. Cathet Cardiovasc Diagn 1995; 34:350-2
2.McGinnity JG, Glazier JJ, Spears JR, Logers C, Turi ZG. Successful redeployment of an unexpanded coronary stent. Cathet Cardiovasc Diagn 1998; 44:52-6.
3.Eggebrecht H, Haude M, von Birgelen C, Oldenburg O, Baumgart D, Herrman J, et al. Nonsurgical retrieval of embolized coronary stents. Cathet Cardiovasc Interv 2000; 51: 432-40.
4.Alfonso F, Martinez D, Hernandez R, Goicolea J, Segovia J, Fernandez-Ortiz A, et al. Stent embolization during intracoronary stenting. Am J Cardiol 1996; 78: 833-5.
5.Colombo A, Maiello L, Almagor Y, Thomas J, Zerboni S, Di Summa M, et al. Coronary stenting: Single institution experience with initial 100 cases using the Palmaz-Schatz stent. Cathet Cardiovasc Diagn 1992; 26: 171-6.
6.Elsner M, Peifer A, Kasper W. Intracoronary loss of balloon-mounted stents: Successful retrieval with a 2 mm "Microsnare" device. Cathet Cardiovasc Diagn 1996; 39: 271-6.
7.Szabo S, Abramowitz B, Vaitkus PT. New Technique of Aorto-Ostial Stent Placement. AJC 2005; 96: 212 H.
8.Applegate R.J, Davis J. M, Leonard JC. Treatment of Ostial lesions using Szabo technique. Ctheter Cardiovasc Interv 2008; 72: 823-8.
9.Holmes DR Jr, Garratt KN, Popma J. Stent complications. J Invasive Cardiol 1998; 10: 385-95.
10.Hoang V, Urban V, Chatelian P, Metz D, Camenzind E, Brzostek T, et al. Randomized evaluation of 6 French Voda-type guiding catheter for left coronary artery angioplasty. Cathet Cardiovasc Diagn 1995; 35: 53-6.
11.Asakura Y, Furukawa Y, Ishikawa S, Asakura K, Sueyoshi K, Sakamoto M, et al. Successful predilation of a resistant, heavily calcified lesion with cutting balloon for coronary stenting: A case report. Cathet Cardiovasc Diagn 1998; 44: 420-2.
12.Rosenblm J, Stertzer SH, Shaw RE, Hidalgo B, Hansell HN, Murphy MC, et al. Rotatinal Ablation of balloon angioplasty failures. J Invasive Cardiol 1992; 4: 312-8.
13.Foster-Smith KW, Garratt KN, Higano ST, Holmes DR. Retrieval techniques for managing flexible intracoronary stent misplacement. Cathet Cardiovasc Diagn 1993; 30: 63-86.
14.Veldhuijzen FL, Bonnier HJ, Michels HR, El Gamal MIH, van Gelder BM. Retrieval of undeployed stents from the right coronary artery: Report of two cases. Cathet Cardiovasc Diagn 1993; 30: 245-8.
Conclusion
”When factory-mounted stent is not a choice”, better manual crimping is required. In case of dislodgement in coronary system if the stent retrieval is not possible then crushing technique could easily and safely be employed. Moreover, better lesion preparation with various techniques prior to stent placement may decrease the incidence of stent dislodgement and embolization.
Introduction
The use of stents during percutaneous coronary intervention is now routine. Stent embolization into the systemic or coronary circulation before deployment is a rare but recognized complication of coronary stenting. It may lead to fatal consequences1-4 including coronary thrombosis and subsequent myocardial infarction.5,6 In the past, manual crimping of stents was associated with a significantly increased risk of stent dislodgement and embolization. Although, manually crimped stents are now rarely used, the problem of stent embolization has not completely been eliminated especially when negotiating tortuous and/or calcified arteries and passage through a previous stent.3 Furthermore, many of the currently available stents are poorly visible on fluoroscopy before and after deployment, therefore, in case of embolization their retrieval becomes more difficult. We report three cases of stent dislodgement that have occurred in our centre during the year 2008 and their management.
Case-1:
A 45-years-old male was admitted in Coronary Care Unit with the diagnosis of Acute Coronary Syndrome. He was hypertensive and known case of chronic stable Angina for last one year. His Coronary Angiogram revealed totally occluded mid Right Coronary Artery (RCA) with good collaterals. Large Ramus branch was severely diseased. Severe ostial disease at Left Anterior Descending (LAD) artery with totally occluded mid segment. Non dominant Left Circumflex (LCX) was also diseased. He had preserved left ventricular (LV) systolic function.
Risks and benefits of surgery and multivessel Percutaneous Coronary Intervention (PCI) were explained to patient and he opted for PCI. After bolus of intravenous Heparin left system was engaged with XB-3 guiding catheter and 0.0014" coronary wire (cougar XT) was advanced in the LAD and another wire in the Ramus branch. Mid LAD and Ramus branch were directly stented with 3.5 x 24 mm (Driver) and 3.0 x 8 mm (Biotronik) successfully. Following which we planned to stent the ostium of LAD and for the proper placement of stent exactly at the ostium we used the Szabo's technique.7,8 The drawback of this technique was to manually crimp the semi-expanded stent. While, trying to place the stent at the ostium it slipped off from the balloon and embolized in the left main. We intertwined it with two coronary wires and tried to pull it in the guiding catheter but unfortunately it did not go inside the catheter and embolized in the left cusp and after a short while in the left main again (Figure-1A). 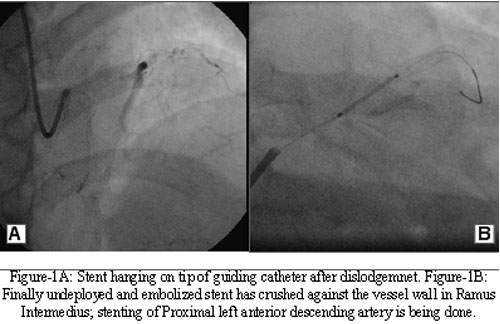
Case-2:
A 65-years-old male, known case of Diabetes mellitus and Hypertension for 10-15 years, presented with CCS-III Angina. His Coronary Angiogram showed moderate ostial disease in LAD, mild lesion in RCA and severe calcified lesion in LCX artery. PCI to LCX artery was decided to reduce the anginal symptoms. Using XB 3.5 guiding catheter and coronary wire (BMW) 0.014", the lesion was predilated with smaller (Sprinter-2.5x15) balloon. To prepare the calcified artery for stenting it was again dilated with a bigger (Cross sail-3.25x15) balloon. Then we took 3.0 x 18 mm (Driver) bare metal stent and when we tried to place it along the lesion, it was obstructed and further advance was not possible probably due to heavy calcification along the lesion. We held the Guiding catheter firmly and gave some gentle jerks to the shaft of the stent, however, the result was a demounted stent with a distorted struts (Figure-2A). 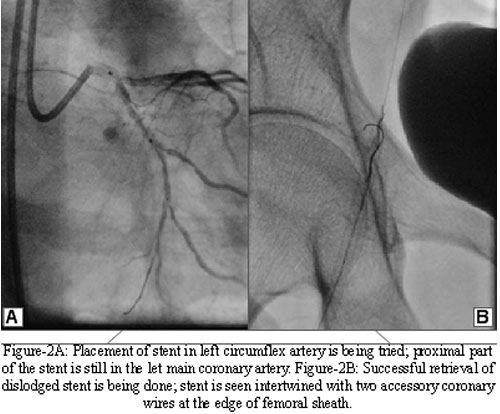
Case-3:
A 35-years-old male with no known co-morbids presented in Emergency Room (ER) with acute antero-septal wall myocardial infarction. Primary PCI was decided and he was brought to the catheterization Laboratory. His angiogram showed critically occluded mid LAD with long bifurcation lesion. Dual antiplatelet therapy and Heparin intravenous bolus was given prior to the procedure and platelet glycoprotein IIb IIIa inhibitor infusion was started. By using JL 3.5 6F guiding catheter, coronary wire and Export catheter a clot was retrieved. The symptoms of the patient improved and TIMI-III flow achieved. We decided to directly stent the vessel and took 3.0 x 30 mm bare metal stent (Driver) and advanced it in the LAD but it stopped progressing midway along the lesion. After, a short while we decided to predilate the vessel and therefore, we tried to retract the stent into the guiding catheter but the stent demounted from the balloon and dislodged. We took another wire and intertwined it with the stent then retrieved the stent in the same fashion as we did in the case 2 (Figure-3A & B). 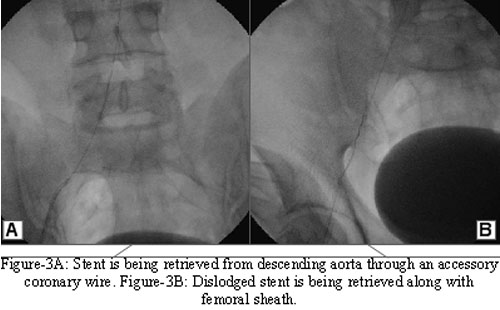
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: