
Abdollah Jafarzadeh ( Department of Immunology, Medical School, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. )
Hamid Bakhshi ( Department of Immunology, Medical School, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. )
Mohammad Taghi Rezayati ( Department of Immunology, Medical School, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. )
Maryam Nemati ( Department of Immunology, Medical School, Rafsanjan University of Medical Sciences, Rafsanjan, Iran. )
November 2009, Volume 59, Issue 11
Original Article
Abstract
Objective: To evaluate the effects of cigarette smoke (CS)-exposed saliva on cellular and antibody responses in an animal model.
Methods: The stimulatory and non-stimulatory saliva samples were collected from 10 healthy subjects and were then exposed to CS for 20 or 80 minutes. The CS-exposed saliva samples were administrated intraperitoneally (i.p) to male Balb/c mice. Then the delayed type hypersensitivity (DTH) and antibody responses to sheep red blood cell (SRBC) was assessed. Moreover, the total white blood cells (WBC) counts and the blood lymphocytes counts were determined.
Results: The mean of DTH responses of animal groups received 20 minutes or 80 minutes CS-exposed saliva samples was significantly lower than that observed in control group. Moreover, The mean titer of anti-SRBC antibody was significantly lower in animal groups who received 80 minutes CS-exposed stimulatory or non-stimulatory saliva as compared to control group (P<0.04 and P<0.002, respectively). The mean counts of blood lymphocytes in 80 minutes CS exposed-stimulatory saliva group was also significantly lower as compared to control group (P<0.05).
Conclusion: These results show that the CS-exposed saliva samples have profound suppressive effects on both cellular and humoral immune response in a mouse animal model (JPMA 59:760; 2009).
Introduction
Presently, about 1.25 billion people are known to be smokers, worldwide and approximately 5 million deaths are attributed to smoking each year.1 It has been reported that cigarette smoke (CS) contains over 4000 different chemicals which influence various organs both locally and systemically.2 One the body systems that is affected by smoking is the immune system.3 The principle function of the immune system is defence against infections and killing of tumour cells.4 It has been reported that cigarette smoking influences both cell mediated and antibody mediated immune responses.3 Accordingly, cigarette smoking was considered as a risk factor for cancers and bacterial-and viral infections.5,6 Although, there is convincing evidence that the CS-contained carcinogens have a direct role in tumorigenesis6 and other mechanisms such as CS-induced immunosuppression may also contribute to increased cancer risk in smokers.
However, it should be noted that there is never a direct exposure between CS and the oral mucosa. Saliva, washes the oral cavity to the larynx and therefore, CS must first interact with saliva before it reaches to the mucosa. Recently, it has been reported that the interaction between CS and saliva may be harmful (instead of protection) and results in the rapid destruction of salivary biological macromolecules, such as enzymes and other proteins.7 In vitro studies have also demonstrated that the saliva has lethal effects on human lymphocytes in the presence of cigarette smoke.8,9 Moreover, a genotoxic activity has been observed in the smokers salivary samples.10
The results of some studies in active smokers or subjects passively exposed to CS, have shown significant alteration in the cellular and humoral immune parameters.3,11 In addition to direct CS-induced immunosuppression, indirect mechanisms may also contribute to immune system disorders. This study conducted for the first time to investigate the effects of CS-exposed stimulatory saliva and CS-exposed non stimulatory saliva on cellular and humoral immune responses in an animal model is to clarify any association.
Materials and Methods
Totally ten healthy non-smoking volunteers (5 males and 5 females, age range 21-27 years) were enrolled in the study. All participants were basically healthy. Subjects with medical history of recurrent infections, acute diseases, history of asthma, allergy, atopic diseases, any suspected immunological disorder and chronic illnesses were excluded from this study. Informed consent was obtained from the participant before enrollment. Moreover, this study was evaluated and approved by the Research Committee of Rafsanjan University of Medical Sciences.
Non-stimulatory and stimulatory saliva were collected from all participants. All saliva samples were collected in the morning between 10 a.m. and 11 a.m to reduce possible circadian interference. Before collecting the saliva, the subjects had no eating or drinking for at least 1 hour. For un-stimulated saliva collection, subjects were asked to generate saliva in their mouths and to spit into a wide test-tube for 10 minutes. Following collection under resting conditions, a stimulated collection of saliva was performed, for which a 2% citric acid solution was applied to the tongue dorsum bilaterally at 30 seconds intervals. The saliva samples were placed on ice and then centrifuged for 15 min at 10,000 gm to remove squamous cells and debris. The resulting supernatant was used for the analysis. It should be noted that we used the combined non-stimulatory and combined stimulatory saliva of subjects for investigation.
The cigarettes used in this study were commercial Winston cigarettes containing 16 mg of tar and 1.1 mg of nicotine (Camel, Winston-Salem, USA). The in vitro exposure of saliva samples to CS has been done according to a method as previously described12 with some modifications. Saliva samples (20 ml of stimulatory saliva or non-stimulatory saliva) were placed in 24-well microplate as 1 ml/well. A Winston cigarette, in which the filter tip was removed, was attached to a vacuum system to draw gasphase cigarette smoke inside sealed 300cm3 flask that the microplate was held in it. After the cigarette smoke was employed, the flasks were incubated for 20 or 80 minutes at 37°C.
Eight weeks male Balb/c mice were purchased from Pasteur Institute, Tehran, Iran. They were given sterilized water and autoclaved standard mouse chow throughout the study. In order to assess the effect CS-exposed saliva on the immunological parameters, mice were divided into 7 groups including control (not exposed to saliva), only stimulatory saliva, only non-stimulatory saliva, 20 minutes CS-exposed stimulatory saliva, 20 minutes CS-exposed non-stimulatory saliva, 80 minutes CS-exposed stimulatory saliva and 80 minutes CS-exposed non-stimulatory saliva. Each groups of animal consisted of 5-7 mice.
Sheep red blood cells (SRBC) were obtained from the Pasteur Institute, Tehran, Iran and preserved in sterile Alsevers' solution. After 3 times washing, the necessary suspension was prepared for priming the animals.
DTH responses was evaluated by priming the mice with 1×108 SRBC injected subcutaneously in the back on day 0. The sensitized animals were challenged with 1×108 SRBC injected subcutaneous on the left hind footpad on day 5. Foot thickness was measured 24 hours later with a Mauser dial caliper and the results expressed as percent of increased foot thickness.13,14 0.2 ml/day of CS-exposed saliva samples (stimulatory or non-stimulatory saliva samples that exposed to CS for 20 min or 80 min) were injected intraperitoneally (i.p.) to each mouse at days 0 to 5.
The antibody responses were assessed by priming mice with 1×109 SRBC injected i.p at day 0. The mice were then bled by intracardiac puncture on day 5 and the antibody responses were assessed. Two fold dilutions of the sera were made in phosphate buffered saline with a total volume of 0.2 ml. Then 0.2 ml volumes of 3% v/v washed SRBC were added to 96 well Nunc microtitre plate. Plates were then incubated at 37°C for one hour and observed for haemagglutination under an inverted microscope. Results were expressed as Log2 titer.13,14 0.2 ml/day of CS-exposed saliva samples (stimulatory or non-stimulatory saliva samples that exposed to CS for 20 min or 80 min) were injected i.p to each mouse at days 0 to 5.
The total cell counts were made by haemacytometer (T-890, Culter USA). Gimsa-stained blood slides were used for differential counts.
Differences in variables were analyzed using t-test, ANOVA, Mann-Whitney U and Kruskal-Wallis tests as appropriate and P values of less than 0.05 were considered significant. All data were analyzed by a computer programme (SPSS, Chicago, IL, USA).
Results
As demonstrated in Figure-1, the mean of DTH responses in animal groups received 20 minutes CS-exposed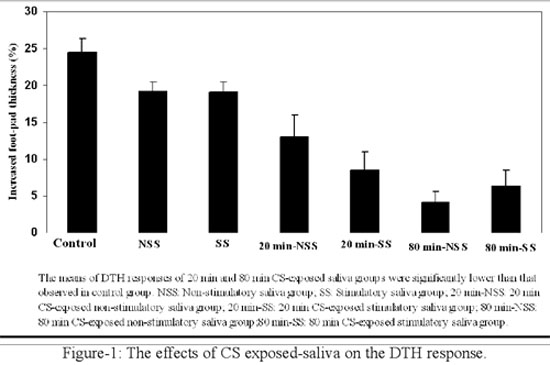
stimulatory saliva group or 20 minutes CS-exposed non stimulatory saliva group were significantly lower than that observed in control group (P<0.0001 and P<0.001, respectively). Similarly, the mean of DTH responses in animal groups administrated 80 minutes CS-exposed stimulatory saliva group or 80 minutes CS-exposed non stimulatory saliva group were significantly lower as compared to control group (P<0.00001). No significant differences were observed between the DTH responses of both unexposed-stimulatory saliva group or unexposed-non stimulatory saliva group in comparison to control group.
The mean titer of anti-SRBC antibody were significantly lower in animal groups that received 80 minutes CS-exposed stimulatory saliva or 80 minutes CS-exposed non-stimulatory saliva as compared to control group (P<0.04 and P<0.002, respectively). The differences of the mean titer of anti-SRBC antibody of animal groups that received 20 min CS exposed-stimulatory saliva or 20 minutes CS-exposed non-stimulatory saliva were not significant from that observed in control group. No significant differences were observed between only stimulatory saliva group or only non-stimulatory saliva group and control group regarding the means titer of anti-SRBC antibody (Figure-2).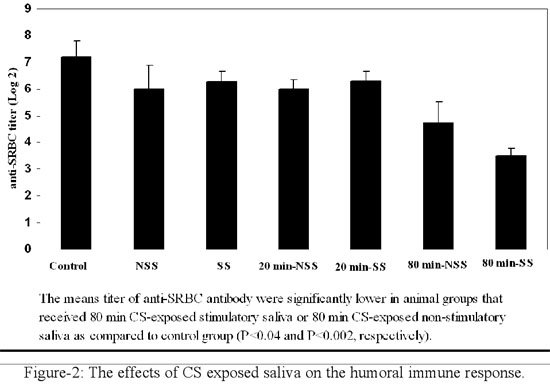
The differences of the mean counts of WBC in animal groups received 20 minutes CS-exposed salivary samples or 80 minutes CS-exposed salivary samples was not significant from that observed in control group, although this parameter was lower in animal groups that received CS-exposed saliva samples. No significant differences were also found between only stimulatory saliva group or only non-stimulatory saliva group and control group regarding the mean counts of WBC.
The mean counts of blood lymphocytes in animal groups received 20 minutes CS exposed-saliva samples or 80 minutes CS exposed non-stimulatory saliva sample were lower than that observed in control group but the differences were not statistically significant. However, the mean counts of blood lymphocytes in 80 minutes CS exposed-stimulatory saliva group (2346 ± 339 cells/mm3) was significantly lower as compared to control group (5038 ± 999 cells/mm3, P<0.05). No significant differences were also found between only stimulatory saliva group or only non-stimulatory saliva group and control group regarding the mean counts of blood lymphocytes.
The mean serum concentration of TGF-b in animal groups received 80 minutes CS-exposed non stimulatory saliva group (128 Pg/ml ± 50.25) was significantly lower than that observed in control group (294.12 Pg/ml ± 49.6; P<0.05). No significant differences was also observed between the mean serum concentrations of TGF-b in animal groups received 80 minutes exposed-stimulatory saliva (276.72 Pg/ml ± 52.3), 20 minutes exposed-stimulatory saliva (291.02 Pg/ml± 27.84) or 20 minutes exposed-non stimulatory saliva (301.92 Pg/ml ± 22.8) as compared to control group. The mean serum concentrations of TGF-b was similarly expressed in only stimulatory saliva group (233.7 Pg/ml ± 56.37) or only non-stimulatory saliva group (238.8 Pg/ml ± 32.6) in comparison to control group.
Discussion
Saliva is armed with various protective mechanisms such as various enzymes, immunological parameters and antioxidant factors that neutralize dangerous substance and therefore provides a protective partition between harmful agents and the mucosal lining of the mouth.15 It has been reported that some components of CS such as unsaturated and saturated aldehydes could interact with thiol-rich substance of saliva, resulting in structural and functional modification of these molecules.16
The results of the present study in an animal model showed that CS-exposed saliva suppresses both cellular and humoral immune responses. These observations are consistent with some immunological disorders reported in cigarette smokers.3 It has been demonstrated that smoking reduces serum levels of immunoglobulins including IgG, IgA and IgM.17 The suppressive effects of smoking on cell mediated immune responses have been also reported.3 It should be noted that the specific immunological functions is mediated by T and B lymphocytes.18 The results of some studies have demonstrated that number of T cell subgroups and the CD4+/CD8+ cells ratio is lower in smokers.19 CS-induced damage to lymphocytes has also been described as anergy, inhibition of some cell functions, genomic deletions and other DNA injuries such as increasing the number of micronuclei formation.20,21 The results of the present study represents that CS may also influence the immune system through indirect mechanisms such as interaction with saliva components. Accordingly CS-induced modifications in salivary components could contribute to CS-related immune disorders. However, the exact mechanism responsible for the immunologic abnormalities induction by CS-exposed saliva remains to be elucidated.
The results of the present study showed that the counts of WBC and blood lymphocytes decreased in CS-exposed saliva groups (especially 80 min CS-exposed stimulatory saliva group). These observations are consistent with other in-vitro studies in which the lethal synergistic effects of CS and saliva on the survival rate of lymphocyte has been reported.8,9 In our previous study, we observed that following 80 minutes exposure of human lymphocytes to CS in the presence of medium supplemented with 30% (v/v) non-stimulatory saliva or stimulatory saliva, the lymphocytes viability significantly decreased to 28.78% and 22.6%, respectively (data not published). Accordingly, it seems that the induction of immunosuppression by CS-exposed saliva may be partly due to CS-exposed saliva induced lymphopenia. Interestingly, the results of our previous and present studies demonstrated that the stimulatory saliva was more cytotoxic as compared to non-stimulatory saliva. One explanation may be that the concentrations of most antioxidant components such as peroxidase, superoxide dismutase and uric acid are lower in stimulatory saliva compared to non-stimulatory saliva which demonstrated by Nagler et al.22 Accordingly, the injurious agents cannot be neutralized by stimulatory saliva and are more cytotoxic. Moreover, it has been shown that human stimulatory saliva contains much higher concentration of iron in comparison to non-stimulatory saliva.22 The higher concentrations of iron in stimulatory saliva could help to explain some of its higher cytotoxicity compared to non-stimulatory saliva. It has been shown that the redox active metals such as iron, in the presence of H2O2 could participate in the Haber-Weiss and Fenton reactions in which harmful reactive hydroxyl free radicals are produced.8 Accordingly it seems that metals may be responsible for the CS-exposed saliva cytotoxicity. Moreover, it has been reported that the addition of potent iron chelator to the saliva prior to exposing the cells to CS, prevented some cellular damages at late phase.23 It has been proposed that an earlier aldehyde attack paves the way for the later metal-related pathways of attack. However, higher toxicity of stimulatory saliva has been attributed to its higher concentrations of iron in comparison to non-stimulatory saliva.22
Both types of saliva were found to have no significant influence on the immunological parameters, alone, if there was no CS exposure. This is not surprising, because saliva is considered as a protective medium against harmful agents such as bacterial, viral, carcinogenic and oxidative substance.15,22
The results of this study also showed that the mean serum concentration of TGF-b of 80 minutes CS exposed-non stimulatory saliva group was significantly lower that that observed in control group. TGF-b produces by a subset of T cells namely regulatory T cells (Treg) that suppress the immune responses.24 These results represent that the CS-exposed saliva induced immunosuppression is a Treg-independent phenomenon. However, the 80 minutes CS-exposed stimulatory or non stimulatory saliva may differentially influence the expression of TGF-b.
In summary, these results showed that the CS-exposed saliva samples have profound suppressive effects on both cellular and humoral immune responses in a mouse animal model. The CS-exposed saliva induced immunosuppression may be partly due to lymphopenia rather than activation of Treg cells.
References
1.Lenney W, Enderby B. "Blowing in the wind": a review of teenage smoking. Arch Dis Child 2008; 93: 72-5.
2.Johnson N. Tobacco Use and Oral Cancer: A Global Perspective. J Dent Educ 2001; 65: 328-39.
3.Pirogowicz I, Gwiazda E, Hoffmann K, Drobnik J, Steclwko A. Cigarette smoking and immunity disorder. Przegl Lek 2007; 64: 886-8.
4.Maplanka C. AIDS: is there an answer to the global pandemic? The immune system in HIV infection and control. Viral Immunol 2007; 20: 331-42.
5.Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med 2004; 164: 2206-16.
6.Hecht SS. Cigarette smoking: cancer risks, carcinogens, and mechanisms. Langenbecks Arch Surg 2006; 391: 603-13.
7.Nagler, Lischinsky S, Diamond E, Drigues N, Klein I, Reznick A. Effect of cigarette smoke on salivary proteins and enzyme activities. Arch Biochem Biophys 2000; 379: 229-36.
8.Hasnis E, Reznick AZ, Pollack S, Klein Y, Nagler RM. Synergistic effect of cigarette smoke and saliva on lymphocytes--the mediatory role of volatile aldehydes and redox active iron and the possible implications for oral cancer. Int J Biochem Cell Biol 2004; 36: 826-39.
9.Hershkovich O, Oliva J, Nagler RM. Lethal synergistic effect of cigarette smoke and saliva in an in vitro model: does saliva have a role in the development of oral cancer? Eur J Cancer 2004; 40: 1760-7.
10.Bloching M, Stephan D, Agha-Mir-Salim P, Berghaus A, Lautenschlager C, Grummt T. Ames test as biomarker. HNO 2001; 49: 440-6.
11.Nakata A, Tanigawa T, Araki S, Sakurai S, Iso H. Lymphocyte subpopulations among passive smokers. JAMA 2004; 291: 1699-700.
12.Greabu M, Battino M, Totan A, Mohora M, Mitrea N, Totan C, et al. Effect of gas phase and particulate phase of cigarette smoke on salivary antioxidants. What can be the role of vitamin C and pyridoxine? Pharmacol Rep 2007; 59: 613-8.
13.Gharegozloo B, Hassan ZM, K Ardestani S, Tavassoli N. Effect of immunomodulator pyrimethamine and cimetidine on immunosuppression induced by burn blister fluid. Iran J Allergy Asthma Immunol 2004; 3: 139-43.
14.Hassan ZM, Ebtekar M. Immunological consequence of sulfur mustard exposure. Immunol Lett 2002; 83: 151-2.
15.Greabu M, Battino M, Mohora M, Totan A, Spinu T, Totan C, et al. Could constitute saliva the first line of defence against oxidative stress? Rom J Intern Med 2007; 45: 209-13.
16.Zappacosta B, Persichilli S, Mordente A, Minucci A, Lazzaro D, Meucci E, et al. Inhibition of salivary enzymes by cigarette smoke and the protective role of glutathione. Hum Exp Toxicol 2002; 21: 7-11.
17.Aral M, Ekerbicer HC, Celik M, Ciragil P, Gul M. Comparison of effects of smoking and smokeless tobacco "Maras powder" use on humoral immune system parameters. Mediators Inflamm 2006; 2006: 85019.
18.Saalmüller A. New understanding of immunological mechanisms. Vet Microbiol 2006; 117: 32-8.
19.Moszczynski P, Zabinski Z, Moszczynski P Jr, Rutowski J, Slowinski S, Tabarowski Z. Immunological findings in cigarette smokers. Toxicol Lett 2001; 118: 121-7.
20.Finette BA, O'Neill JP, Vacek PM, Albertini RJ. Gene mutations with characteristic deletions in cord blood T associated with passive maternal exposure to tobacco smoke. Nat Med 1998; 4: 1144-51.
21.Singh SP, Kalra R, Puttfarcken P, Kozak A, Tesfaigzi J, Sopori ML. Acute and chronic nicotine exposures modulate the immune system through different pathways. Toxicol App Pharmacol 2000; 164: 65-72.
22.Nagler RM, Hershkovich O, Lischinsky S, Diamond E, Reznick AZ. Saliva analysis in the clinical setting: revisiting an underused diagnostic tool. J Invest Med 2002; 50: 214-25.
23.Reznick AZ, Hershkovich O, Nagler RM. Saliva - a pivotal player in the pathogenesis of oropharyngeal cancer. Brit J Can 2004; 91: 1-8.
24.Wilczynski JR, Radwan M, Kalinka J. The characterization and role of regulatory T cells in immune reactions. Front Biosci 2008; 13: 2266-74.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: