
Arsalah Raffat ( Department of Orthodontics, Fatima Jinnah Dental College, Karachi )
Waheed ul Hamid ( Orthodontic Department, deMontmorency Institute of Dental Sciences, Lahore. )
November 2009, Volume 59, Issue 11
Original Article
Abstract
Objective: To evaluate the dentofacial morphology of adenoidal faces via linear and angular measurements on lateral cephalometric tracings and compare the extent of changes with control group.
Methods: A cross sectional study was conducted from January to July 2007 at the Department of Orthodontics, de'Montmorency Institute of Dental Sciences/Punjab Dental Hospital, Lahore (tertiary health center). As a non probability purposive sampling, total of 90 cephalometric radiographs of subjects (12 to 17 years of age) 45 with adenoidal faces and 45 subjects having normal class I and orthognathic profile were collected and utilized in the study. Subject with cranio-facial anomalies and syndromes, history of previous orthodontic treatment or trauma to the head and neck region were excluded. The collected data was entered on SPSS version 10 and analyzed by using, Paired 't' test.
Results: Significant difference is seen among the readings showing a drastically vertical pattern of growth in dentofacial complex, except the palatal inclination angle.
Conclusion: The findings suggest that the subjects with upper airway obstruction display excessive vertical dentofacial development, leading to a long face appearance. The condition needs to be prevented by early recognition and treatment of the causative factor (JPMA 59:747; 2009).
Introduction
Nasal breathing is the first physiological function developed at birth. Responsible for the process of air conditioning, warming, humidification and filtering, it also serves as protection for respiratory tract. Moreover it has effects on development and determination of dentofacial morphology.1 The adenoid is a hypertrophied lymphoepithelial tissue that comprises part of Waldeyer's pharyngeal ring and plays an important role in the immune system.2 Adenotonsiller hypertrophy causes upper airway obstruction and may lead to pulmonary alveolar hypoventilation, pulmonary hypertension, symptoms like chronic mouth breathing, loud snoring, obstructive sleep apneas, excessive daytime sleepiness, and even cor pulmonale.3,4
In this situation, a number of postural changes, such as open mandible posture, downward and forward positioning of the tongue, and extension of the head, can take place.
Oral respiration alters the muscle forces exerted by the tongue, cheeks, and lips upon the maxillary arch. Intraorally, the dentist might expect to find a narrow maxillary arch with a high palatal vault, a posterior crossbite, a Class II or III dental malocclusion, and an anterior open bite.5
Studies have demonstrated by rhinomanometric tests, that a significant relationship occurs between a smaller distance of Adenoid-Posterior Nasal Spine or impaired nasal breathing and a wide craniocervical angulation and forward inclination of the cervical spine.6,7If these postural changes continue for a long period, especially during the active growth stage, dentofacial disorders at different levels of severity occur, together with the inadequate lip structure and long face syndrome/adenoidal faces.
Adenoidal face is described as long lower third facial height, narrow alar bases, lip incompetence, a narrow or "V" shaped maxillary arch, and greater than normal mandibular plane angle.3,4 Timing of the removal of excessive adenoid tissue plays an important role on the recovery of this undesirable craniofacial growth pattern.8 A valid diagnostic agreement between endoscopic and radiologic findings has been found in observing the severity of adenoidal hypertrophy and in particular, the patency of the nasopharyngeal space.9
Roentgenography and eventually cephalometrics provided orthodontists with an ability to see beneath soft tissue, which gave them greater insight into most of the hard and soft anatomical structures that contribute to facial growth and development.3
Different cephalometric methods have been used in the past to assess the saggital skeletal discrepancy.10-12 Some authors have evaluated the patency of the upper airways using cephalometric techniques and has established a connection between the reduction of the nasopharyngeal space and the increase of the craniocervical angle.13 Documentation of several studies suggest an ongoing change in head posture possible by a change in the mode of breathing from oral to nasal via adenoidectomy or tonsillectomy surgery by Otolaryngologist14-17 with or without immunotherapy (commonly referred to as "allergy shots")4 and orthodontic intervention like rapid maxillary expansion (RME).18 RME is able to increase the capacity of the nasopharyngeal airways and leads to significant changes in the cranio-cervical angles,19 thereby contributing to a change in craniofacial development and relative reduction in vertical dimension.
This study puts an emphasis on the early intervention to prevent the skeletal and dental disfigurement due to disturbance in skeletal development, abnormal muscular growh or poor positioning of the anterior teeth caused by buccal habits.20 Therefore, improve the quality of life style, by decreasing the problem of obstruction in nasal airway leading to restlessness at night, behavioral problems, poor school performance and day time sleepiness,3 also by lowering the incidences of complexities of dentofacial treatments i.e. unsuccessful orthopaedic treatment which may require orthagnathic surgery at an older age. Therefore this study has helped to evaluate the extent of deformation of skeletal pattern in the established adenoidal cases, to get a clear picture for methods of prevention.
The aim of this study was to compare the extent of difference in dentofacial morphology between adenoidal faces and control group with the help of lateral cephalogram.
Patients and Methods
A cross sectional study was conducted for a period of 6 months from January to July 2007 in Department of Orthodontics, de`Montmorency Institute of Dental Sciences / Punjab Dental Hospital Lahore (Tertiary health center).
The subjects selected for this study included diagnosed 45 subjects with adenoidal faces by Otolaryngologist and 45 subjects having normal class I and orhthagnathic profile (
It was a Non Probability Purposive sampling and the subjects with in criteria were selected and an informed consent was taken. Biodata, history and cephalometric readings were collected on the pre-designed proforma. The radiographs were taken with the subject standing in Natural Head Position as described by Sahin Saglam AM et al. 21 Cephalometric film tracings was made on acetate sheets and data collected by using cephalometric landmarks i.e.
S: Sella point: midpoint of sella turcica, determined by inspection.
Se: Midpoint of the entrance to the sella.
N: Nasion: The intersection of the internasal structure with the nasofrontal structure in the midsagital plane.
Go: Gonion: The point on the jaw angle, which is the most inferiorly, posteriorly and outwardly directed.
Gn: Gnathion: The most inferior point in the contour of the chin.
Me: Menton: The lowermost point on the shadow of the symphysis.
Ar: Articulare: A constructed point representing the intersection of cranial base and the posterior outlines of the ascending rami or mandibular condyles.
PTM: Pterygomaxillary fissure: a bilateral, inverted teardrop-shaped radiolucency, whose anterior border represents the posterior surfaces of the tuberosities of the maxilla.
ANS: Anterior nasal spine: tip of anterior nasal spine.
PNS: Posterior nasal spine: tip of posterior spine of palatine bone in hard palate.
S: Bjork's sum of posterior Inner angles: The sum of three posterior angles (Saddle, Articular and Gonion) measured on an average was 396 ± 5.
PP: Palatal Plane: A line joining PNS to ANS.
Pn-Line: Pn-Line: Perpendicular on the Se-N line at Point N' (= Point located 8mm anterior to point N) extended downward to the palatal plane.
The millimetric measurements (as illustrated in Figure) were recorded by using digital vernier caliper to calculate ratios and included:
1. S-Go/N-Me (PFH/AFH)
2. ANS-Me/N-Me (LPH/AFH)
3. N-ANS/ANS-Me (UFH/LFH)
The angles taken for skeletal assessment included:
1. SN-GoGn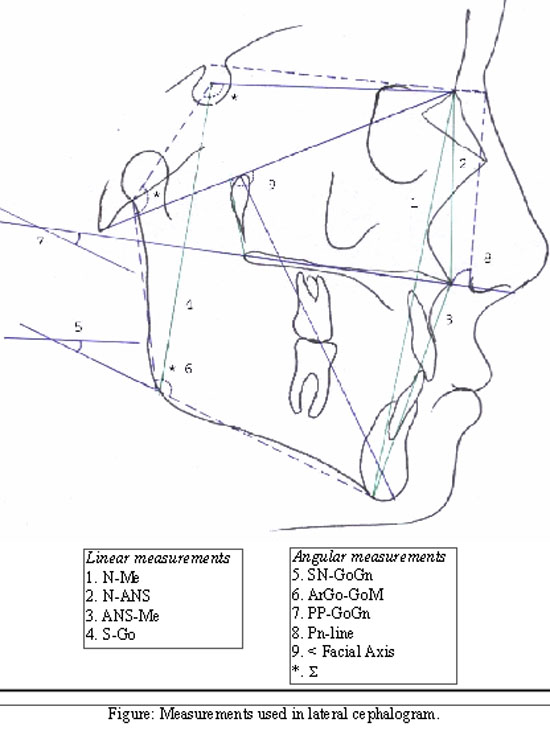
2. Ar.Go-GoMe
3. PP-GoGn
4. Bjorks polygon
5. Max inclination
6. Facial Axis
The measurements were specially chosen to relate the skeletal structures as angles or as ratios to prevent the magnification error of the radiographs. The collected data was analyzed by SPSS version 10. Independent sample t-test was applied to compare mean difference between groups for linear and angular measurements, to see the extent of skeletal derangements.
Duplicate determinations were also carried out for all the linear and angular variables measured on the 25 radiographs, selected at random and repeated by the same orthodontist. The measurements were undertaken 2 weeks apart to remove human error, no significant difference was found using Paired't' test. P-value less than and equal to 0.05 was considered significant.
Results
The group statistics obtained for all the variables (Table-1) indicates mean values with Std. Deviation.
When adenoidal faces were compared with the control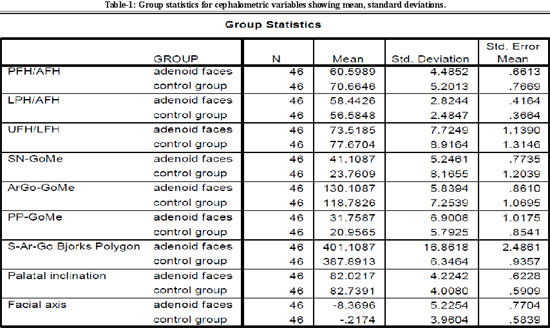
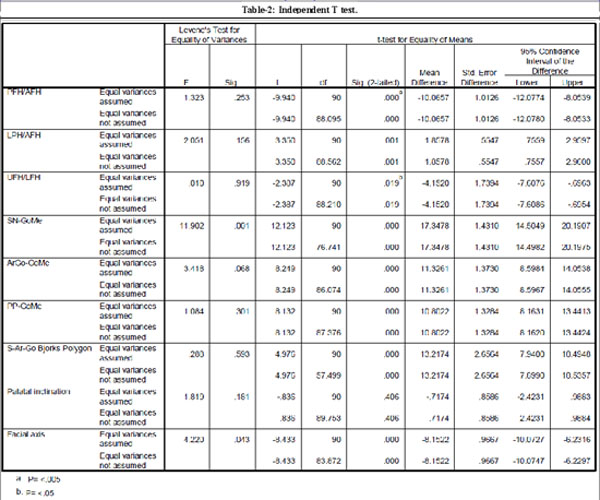
group (Table-2), most of the readings presented were significantly greater: and included PFH/AFH (P <.005) with mean difference of-10.06, LFH/AFH (P <.005) 1.85, SN-GoMe (P <.005) 17.3, ArGo-GoMe (P <.005) 11.3, PP-GoMe (P <.005) 10.8, S-Ar-Go (P <.005) 13.217 and Facial axis (P <.005) -8.15. Significance level (P<.05) was observed for UFH/LFH with mean difference of -4.15. Palatal inclination was the only factor that presented nonsignificant result and had a mean difference -0.71.
Discussion
Subtenly22 used serial Cephalometric head films to study the adenoid growth pattern and found the peak mass size at the age of 10-15 years. The study had no sexual dimorphism, still it guides for the time period till the adenoid can effect the growth pattern. The growth of adenoid progressively regresses and usually atrophies by adulthood.
According to Meredith23 the growth of the face (excluding the mandible) is completed at an early age. 60% of craniofacial development takes place during the first 4 years of life and 90% by age 12.
Otolaryngologists are increasingly being asked to objectively evaluate the nasal airway of pediatric patients. This is in part due to recent interest in snoring, sleep apnoea, nasal obstruction and as it relates to orthodontic deformities leading to early surgical removal of adenoids.
This study cannot be compared to most of different studies, where the age taken was 7-10 years,20 11-12 years,8 8.8 years on average15 or compared the pre and post surgical changes8,17 in the growth of the facial pattern, in contrast the present study used developed adenoid faces and non growing patients.
Development of adenoidal faces showed the extremes of deviation from normal, explained by the Linder Aronson's remark that increase in lower facial height is independent of other skeletal units and dependent upon the growth direction of the mandible and neuromuscular factors influencing mandibular posture.8
Development of mandible is not completed at around 18 years, if the problem is coped a an early age — that is, before the permanent teeth are positioned — the prevention of an orthodontic problem is possible.
However, once the habit is established and the denture is procumbent, then the improvement of breathing may be of little advantage since the denture relationships may prevent closure of the lips.22 Therefore the data taken was of 12 to 18 years of age, with emphasis on the "established adenoidal faces" to evaluate the extremes of deformity that may be observed, i.e. increased then normal facial axis and S presenting clockwise rotation of the mandible.24,25
The results of Bjork's polygon presents an increase in facial height and thus referring to the open bite tendency of lower facial development similar to most of the studies in literature and is complemented by the results of ratio between posterior and anterior facial heights (PFH/AFH) and upper and total anterior facial heights (UFH/LFH).
According to Bjork, genetic and environmental factors which stimulate the vertical growth of the molar region, which are not compensated by condylar growth, result in an anterior open bite.20
Nonsignificant results of palatal inclination (mean difference -0.7174) suggest normal maxillary growth in vertical plane i.e. no difference from the control group, others have shown counter clockwise where anterior nasal spine was superiorly positioned20 and presented anterior open bite.
In most of the studies the reason of excess facial height is said to be "buccal habit"20 i.e. prolonged period of oral respiration leading to extensive eruption of the posterior molars, in response to a lack of occlusal contact.
The insignificant results of palatal inclination angle conforms to the statement therefore making it a buccal dentoalveolar defect in the vertical plane, causing a wedge effect to mandibular growth in clockwise direction, the results are conforming if based on these observations and other studies8 as there is highly significant difference of maxillo-mandibular angle, sella nasion-mandibular plane angle and gonial angle observed among control and adenoidal faces.
Conclusions
The results of study show highly significant differences of skeletal pattern between controls and adenoidal faces. Significantly high angle profile and the vertical pattern of growth indicate a combination of orthodontic and maxillofacial surgery for treatment of such cases. We must be familiar with the dentofacial development and basic concepts of intervention to provide optimal care for our paediatric patients. Earlier detection and intervention is necessary to prevent adenoidal features. For evaluation of children with nasal obstruction and dental abnormalities it is imperative that a multidisciplinary approach and cooperation between the paediatricians, orthodontists and Otolaryngologist is maintained.
Acknowledgements
We thank Dr Irfan (Orthodntist at Punjab Dental Hospital Lahore) for his helpful advice and we are greatful to Professor Dr Arif Tarrar (head of ENT depart. Ch & ICH Lahore) for the enthusiastic participation in this study and his guidance on the subject.
References
1.Filho DI, DaSilva NB. Orthodontic diagnosis of nasopharyngeal obstruction. J Clinical Orthod 2005; 6:371-4.
2.Imamura N, Ono T, Hiyama S, Shiwata YI, Kuroda T. Comparison of the sizes of adenoidal tissues and upper airways of subjects with and without cleft lip and palate. Am J Orthod Dentofacial Orthop2002; 122: 189-94.
3.Salam OH, Briss BS, Annino DJ. Nasorespiratory function and craniofacial morphology-A review of the surgical management of the upper airway. Semin Orthod 2004; 1:54-62.
4.Lampasso JD, Lampasso JG. Allergy, nasal obstruction, and occlusion. Semin Orthod 2004; 1:39-44.
5.Cazzolla AP, Campisi G, Lacaita GM, Cuccia AM, Ripa A, Testa NF, et al. Changes in pharyngeal aerobic microflora in oral breathers after palatal rapid expansion. BMC Oral Health 2006; 6:2
6.Huggare J, Laine-Alava MT. Nasorespiratory function and head posture. Am J Orthod Dentofacial Orthop 1997; 112: 507-11.
7.Solow B, Skov S, Ovesen J, Norup PW, Wildschiotdz G. Airway dimensions and head posture in obstructive sleep apnoea. Eur J Orthod 1996; 18: 571-9.
8.Arun T, Isik F, Sayinsuk. Vertical growth changes after adenoidectomy. Angle Orthod 2003; 73:146-50.
9.Filho DI, Raveli DB, Raveli RB, Loffredo LC, Gandini LG. A comparison of nasopharyngeal endoscopy and lateral cephalometric radiography in the diagnosis of nasopharyngeal airway obstruction. Am J Orthod Dentofacial Orthop 2001; 120: 348-52.
10.Waheedul-Hamid, Asad S. Prevalence of skeletal components of malocclusion using composite cephalometric analysis. Pak Oral Dent J 2003; 23; 137-44.
11.Firdos T, Waheedul-Hamid, Asad S.ANB+AOBO Zone Index (Applicability to Pakistani population) Pak Oral Dent J 2004; 24:193-6.
12.Ijaz A. A cephalometric study to identify classification of malocclusion in patients attending orthodontic unit of the dental section at CH&ICH Lahore. JPDA 2004; 13:130-8.
13.Solow B, Siersbaek-Nielsen S, Greve E. Airway adequacy, head posture, and craniofacial morphology. Am J Orthod 1984; 86: 214-23.
14.McGuinness NJ, McDonald JP. Changes in natural head position observed immediately and one year after rapid maxillary expansion. Eur J Orthod.2006; 28:126-34.
15.Tecco S, Festa F, Tete S, Longhi V, D'Attilio M. Changes in head posture after rapid maxillary in mouth-breathing girls: a controlled study. Angle Orthod. 2005; 75:171-176.
16.Woodside DG, Linder-Aronson S, Lundstorm A, McWilliam J. Mandibular and maxillary growth after changed mode of breathing. Am J Orthod Dentofacial Orthop 1991; 100: 1-18.
17.Rahber R. Adenotonsiller Hypertrophy: The presentation and Management of upper airway obstruction. Semin Orthod 2004; 10:244-6.
18.Mahony D, Karsten A, Linder-Aronson S. Effects of adenoidectomy and changed mode of breathing on incisor and molar dentoalveolar heights and anterior face heights. Aust Orthod J 2004; 20:93-8.
19.Linder-Aronson S, Woodside DG, Lundstorm A. Mandibular growth direction following adenoidectomy. Am J Orthod Dentofacial Orthop 1986; 89: 273-84.
20.Wenzel A, Henriksen J, Melsen B. Nasal respiratory resistance and head posture: effect of intranasal corticosteroid (Budesonide) in children with asthma and perennial rhinitis. Am J Orthod 1983; 84: 422-6.
21.Sahin SAM, Uydas NE. Relationship between head posture and hyoid position in adult females and males. J Craniomaxillofac Surg 2006; 34: 85-92.
22.Subtelny AR. The significance of adenoid tissue in orthodontia.Angle. Orthod 1954; 24: 59-69.
23.Meridith HV. Growth in head width during the first twelve years of life. Pediatrics1953; 12: 411-29.
24.Kawashima S, Peltomaki T, Sakata H, Mori K, Happonen R-P, Ronning O.Craniofacial morphology in preschool children with sleep-related breathing disorder and hypertrophy of tonsils.Acta Paediatr 2002; 91: 71-7.
25.Behlfelt K. Enlarged tonsils and the effect of tonsillectomy. Characteristics of the dentition and facial skeleton. Posture of the head, hyoid bone and tongue. Mode of breathing. Swed Dent J Suppl 1990; 72: 1-35.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: