
Seema Hasnain ( Department of Community Medicine, Allama Iqbal Medical College, Lahore. )
Naheed Humayun Sheikh ( Department of Community Medicine, Allama Iqbal Medical College, Lahore. )
October 2009, Volume 59, Issue 10
Original Article
Abstract
Objective: To assess the knowledge and practices among the diabetic patients regarding foot care.
Methods: In this cross sectional study, by using non-probability convenience sampling, 150 diabetic respondents fulfilling the inclusion criteria were included in the study. Their knowledge and practices regarding foot care were assessed by a pre-tested questionnaire and classified as good, satisfactory and poor depending upon the score. Fifteen questions each were asked regarding knowledge and practices of foot care. Each question was assigned one mark. If score was more than 70% (11-15), it was regarded as good, if score was 50-70% (8-10) it was regarded as satisfactory and if score less than 50% (<8) it was regarded as poor both for knowledge and practice for foot care.
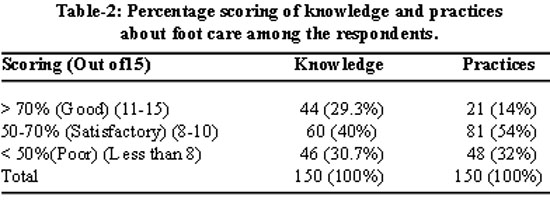
Results: The mean age of the respondents was 48 ± 10.8years. About 29.3% respondents had good knowledge, 40% had satisfactory knowledge and 30.7% had poor knowledge about foot care. Whereas only 14% respondents had good practices for foot care, 54% had satisfactory practices and 32% had poor practices. Education of the respondents had significant statistical association with knowledge (p-value<0.001) and practices (p-value <0.001) regarding foot care. Sex and income per capita had shown no significant statistical association with knowledge and practices regarding foot care.
Conclusion: About one third of diabetic patients had poor knowledge about foot care and only very few patients had good practices for foot care. Literacy has significant association with the knowledge and practices related to foot care in diabetic patients (JPMA 59:687; 2009).
Introduction
Diabetes Mellitus is a syndrome of chronic hyperglycaemia due to relative insulin deficiency, resistance or both. About10-15% of diabetic patients develop foot ulcers at some stage in their lives. Diabetic foot problems are responsible for nearly 50% of all diabetes related hospital admission.1
Diabetes currently affects about 200 million people worldwide and is expected to reach 333 million by 2025, with most of the massive burden falling in developing countries. Every year 3.2 million deaths are attributable to the disease, no matter where people are from and where they live. However, many people are more vulnerable because they do not have access to appropriate health care and education. Poverty and social exclusion increase the risks of developing diabetes, the complications associated with the disease and dying as a consequence of diabetes.2
According to the International Diabetes Federation (IDF)
Foot ulcers are among the most common complications of diabetes with prevalence of 4-10%. They become infected frequently, can be expensive to treat and usually are the first step towards amputation of a lower extremity.5 It has been shown that 49-85% of all diabetic foot related problems are preventable if appropriate measures are taken. This can be achieved through a combination of good foot care — provided by a multidisciplinary diabetes care team and appropriate education for both people with diabetes and health care professionals.6 All patients with diabetes are potentially at risk from diabetic foot which can only be avoided by creating awareness about the importance of appropriate self care.
Diabetologists started recognizing diabetic foot problems in
According to the American Diabetes Association, there are certain guidelines to be followed by diabetic persons.9 This study was carried out to assess the knowledge and practices among the diabetic patients regarding foot care.
Methods
A cross-sectional study was conducted in the diabetic clinic situated in outpatient department of Jinnah Hospital Lahore. The average number of patients visiting diabetic clinic is more than 1300 per month. The inclusion criteria for the cases included diagnosed cases of type I and II diabetes since at least six months, who had never developed foot ulcers. Sample size was calculated through computer software program Epi Info 6.2. The number of diabetic patients visiting Diabetic clinic is 15,877 annually. Prevalence of diabetes is 10% and at 95% confidence interval with margin of error of 5%, the minimum representative sample was 137 but we took 150 respondents. Non-probability convenience sampling technique was utilized for this study. The respondents were interviewed on a pre-tested structured questionnaire after their verbal consent. The dependent variables of the study were knowledge and practices regarding foot care in diabetics and the independent variables were education, occupation and income per capita. There were six teams comprising of two female students and one male student of 4th year MBBS class. Each team interviewed 5 diabetic patients each day. The responses were read out by the data collectors from the pre-tested close ended questionnaire.
Data was analyzed by using SPSS version 11. Simple frequency distribution tables were generated for dependent and independent variables. Chi-square test was applied to find out whether there is any statistical significant effect of socioeconomic factors on knowledge and practices regarding foot care in diabetics. Fifteen questions each were asked regarding knowledge and practices of foot care. Each correct answer was given one mark.
Good knowledge: If score is more than 70% (11-15)
Satisfactory knowledge: If score is 50-70% (10-8)
Poor knowledge: Scores less than 50% (<8)
Good Practices: If score is more than 70% ranging from (11-15)
Satisfactory practices: If score is between 50-70% (10-8).
Poor practices: Score less than 50% (<8).
Results
A total of 150 respondents were selected. The mean 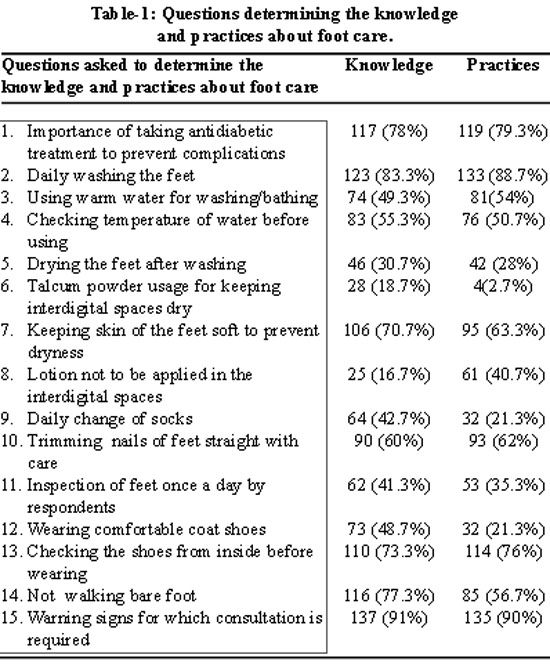
A total of 117 respondents (78%) knew the importance of keeping the blood glucose level within normal limits to prevent themselves from its complications and 119 (79%) were taking the antidiabetic treatment regularly. The knowledge and practices regarding foot care is approximately 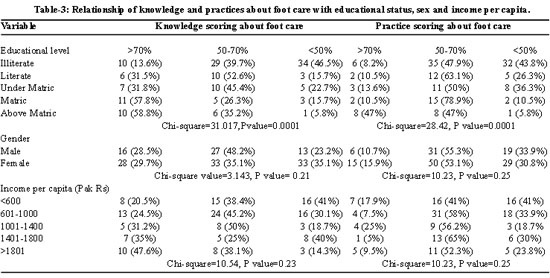
The role of education has shown an impact on the knowledge (p=0.0001) and practices (p=0.0001) regarding foot care. Sex was not significantly associated in relation to knowledge (p=0.21) and practices (0.25) regarding foot care. Similarly income per capita has shown no association with the knowledge (0.23) and practices (0.25) regarding foot care (Table-3).
Discussion
This study was conducted to assess the knowledge and practices of the diabetic patients on foot care. Regarding knowledge, only 29% respondents had good information (>70%) about foot care and formal education had a role in better knowledge about foot care. In this study, there were 34 respondents who were illiterate and their score was <50% and 21 respondents whose educational qualifications were matric and above matric, their score regarding knowledge was more than >70%. In a study conducted in India, which concluded that low scores were common with poor formal education, thus confirming relationship between education and knowledge.10 Role of formal/school education is further confirmed by a study from Italy where the presence of foot complications was correlated with insulin treatment, cigarette smoking and low levels of school education.11 School education has also shown positive relationship with good practices. In the present study, 54% of the respondents had satisfactory practices regarding foot care, 32% had poor practices and only 14% had good practices. Sex has shown no relationship regarding knowledge and practices of foot care whereas in above referred study conducted in India, low scores for foot care knowledge were more common in women (78.5%) than in men (62.5%). However this can be explained on the basis that in that particular study, there were more women with low educational status.10 It can be deduced that the results are consistent with our study. Thus education has a strong relationship with knowledge and practices about foot care. Whereas in another study, multivariate analysis showed that age, years of schooling and sex were independent determinants of the knowledge score in the respondents with type 2 Diabetes.12
The role of physicians is very important in improving the knowledge and practices regarding foot care. In a study from
This recent study reveals that only 14% of the respondents had good practices for foot care and 32% had poor foot care practices which indicates an alarming situation and one should take appropriate action for it. It does not require costly measures but simple preventive measures to prevent the persons to suffer from disability. Another striking feature which is revealed in this study is that 40% of the respondents had satisfactory knowledge (50-70%) whereas 54% of the respondents had satisfactory practices (50-70%) regarding foot care. This 14% increase in practices with less knowledge indicates that people are doing good practices without knowing that they are good for health. This may be explained on the basis of Islamic rituals which they are performing religiously without knowing that some of these activities are a part of good foot care practices e.g. most of the respondents (83.3%) had the knowledge of washing feet daily and 88.7% of the respondents were practicing washing of the feet as they did ablution before offering prayers. Similarly 73.3% of the respondents answered that they had the knowledge to always check the shoes before wearing that it may not have any insect or tiny gravels and regarding practice 76% of the respondents always checked their shoes before wearing. The possible reason for this difference in knowledge and practice could be our religious principles.
This study has shown a marked gap in the knowledge and practices of the diabetic patients regarding foot care in a diabetic clinic of a tertiary level hospital. This also reflects indirectly a grim situation in the primary and secondary health care facilities. Diabetic foot is one of the main complications of Diabetes Mellitus of high socioeconomic impact, characterized by foot lesions and finally leg amputation in most of the cases. Foot care education is the most crucial tool for preventing lower leg amputation. Thus low cost, low technology evaluation and preventive processes are enough to substantially reduce the rates of risk. An individualized educational intervention can lead to improved foot care knowledge; self care practices and confidence in performing foot related self care. There is a need to reorient and motivate health personnel in educating diabetics about self care and also practicing by themselves proper foot examination when and where required. Print and electronic media must be engaged in order to enhance the public awareness of diabetes and its complications. Strategies must be worked out to develop a countrywide network of diabetes centers with implementation of primary prevention programs regarding foot care.
Acknowledgement
The authors express their sincere thanks to the Prof. Syed Sibt-ul-Hasnain, Ex-Principal of
References
1.Kumar P, Clark M. Diabetes Mellitus and other disorders of metabolism. Kumar & Clark Clinical Medicine.
2.International Diabetes Federation Press release Karachi, Pakistan-26 February 2006 - Diabetes kills without distinction. (Online) 2009 (Cited 2007 June 15). Available from URL: http://www.idf.org/home/index.cfm?unode=DE93DC2D-468B-4C75-91DA-69314504BD0E.
3.International Diabetes Federation: Diabetes Atlas 2006.
4.Shera AS, Rafique G, Khawaja IA, Ara J, Baqai S, King H. Pakistan national diabetes survey: prevalence of glucose intolerance and associated factors in Shikarpur, Sindh Province. Diabet Med 1995; 12: 1116-21.
5.
6.Bakker K, Riley P. The year of the diabetic foot. Diabetes Voice 2005; 50: 11-4.
7.Bakker K. Multidisciplinary team managing diabetic foot has amputations by 34% which is quite impressive (Interview). Pulse International 2006; 7: 1-2.
8.Jawaid SA, Jawaid M. Management of diabetic foot ulcers: some bitter facts and harsh realities.Pak J Med Sci 2006; 22 : 97-100.
9.http://familydoctor.org/online/famdocen/home/common/diabetes/living/352.html. [Cited 2007 May 15].
10.Viswanathan V, Shobhana R, Snehalatha C, Seena R, Ramachandran A. Need for education on foot care in diabetic patients in India. J Assoc Physicians
11.De Beradis G, Pellegrini F, Fanciosi M, Belfiglo M, Di Nardo B, Greenfield S, et al. Are Type 2 diabetic patients offered adequate foot care? The role of physician and patient characteristics. J Diabetes Complications 2005; 19: 319-27.
12.Murata GH, Shah JH, Adam KD, Wendel CS, Bukari SU, Solvas PA, et al. Factors affecting diabetes knowledge in Type 2 diabetic veteran. Diabetologia 2003; 46: 1170-8.
13.Corbett CF. A randomized pilot study of improving foot care in home health patients with diabetes. Diabetes Educ 2003; 29: 273-82.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: