
Seema Bibi ( Department of Obstetrics & Gynaecology, Liaquat University of Medical & Health Sciences, Jamshoro, Hyderabad, Pakistan. )
Saima Ghaffar ( Department of Obstetrics & Gynaecology, Liaquat University of Medical & Health Sciences, Jamshoro, Hyderabad, Pakistan. )
Mohammad Ali Pir ( Department of Obstetrics & Gynaecology, Liaquat University of Medical & Health Sciences, Jamshoro, Hyderabad, Pakistan. )
Sajida Yousfani ( Department of Obstetrics & Gynaecology, Liaquat University of Medical & Health Sciences, Jamshoro, Hyderabad, Pakistan. )
October 2009, Volume 59, Issue 10
Original Article
Abstract
Objective: To determine frequency, obstetrical risk factors and the subsequent feto-maternal outcome in women suffering from placental abruption.
Methods: A retrospective case series study was carried out in the Department of Obstetrics and Gynaecology Unit One, Liaquat University Hospital Hyderabad, Pakistan from 1st January 2006 to 31st December 2006. All women with the diagnosis of placental abruption having more than 24 weeks gestation were included in the study.
Results: Of the 2224 delivered women 106 (4.7%) had placental abruption. All of the 106 women were un-booked, with 67 (63%) in the age group 20-35 years, 68 (64%) belonged to rural areas. 98 (92%) patients were multiparous and 57 (54%) were preterm. The commonest medical disorders observed were anaemia in 84 (79%), Diabetes Mellitus in 8 (8%) and gestational hypertension in 8 (8%) patients. There were five maternal deaths, showing case fatality rate of 5%. The foetal prognosis was characterized by low birth weight seen in 74 (70%), low apgar score in 30 (28%) and high still birth rate in 54 (51%), constituting perinatal mortality rate of 25.62/1000 deliveries.
Conclusion: Abruptio placentae is associated with adverse maternal and foetal outcome. Multiparity, un-booked status, rural residence and maternal anaemia are important risk factors (JPMA 59:672; 2009).
Introduction
Abruptio placentae is uterine bleeding from the premature separation of the normally sited placenta after 20 weeks of gestation. Its exact etiology remains obscure, however various risk factors have been implicated like advanced maternal age, high parity, low socio-economic status, smoking, folic acid deficiency, maternal hypertension, thrombophilia and trauma.1
It is a high risk situation not only for the mother but also is a significant cause of perinatal loss. The maternal consequences are secondary to the severity of placental abruption. The foetal effects are also determined by the severity of placental abruption, gestational age and underlying risk factors like intra-uterine growth restriction. In the developed world, the frequency has been reported from 0.43% to 1.8% with perinatal mortality ranging from 4.4 to 67.3%.2 In Pakistan, it ranges from 2.2% to 7% with alarmingly high perinatal mortality of 50.63% to 62.5%.3-5
The objective of the study was to determine the frequency, obstetrical risk factors and the subsequent foeto-maternal outcome in women suffering from placental abruption.
Patients and Methods
It was a retrospective case series study carried out at the Department of Obstetrics and Gynaecology Unit One, Liaquat University Hospital Hyderabad, Pakistan from 1st January 2006 to 31st December 2006. All women with the diagnosis of placental abruption and having more than 24 weeks gestation were included in the study. Data was collected on pre-designed Performa from the patient's records and results were analyzed.
Results
Out of total 2224 deliveries at Gynaecology Unit One, Liaquat University Hospital Hyderabad, 151 women had antepartum haemorrhage. Placental abruption was observed in 106 cases, which corresponds to the frequency of 4.7% while rest of the cases belonged to placenta previa and other incidental causes.
All were un-booked cases and majority 68 (64%) were referred from rural areas of Sindh. Sixty seven (63%) women were in age group of 20 to 35 years while 38 (36%) were more than 35 years of age. There were 98 (92%) multiparous women with grandmultipara constituting half of the study population. Gestational age was less than 36 ± 6 weeks in 57 (54%) cases, and nearly half of them were having less than 32 weeks pregnancy. About half of the study group presented with abruption, which was severe enough to cause intra-uterine foetal demise. Caesarean delivery was required in 29 (27%) women. In 21 (81%) women, operation was performed in foetal interest while in 5 (19%) women surgery was needed due to severe abruption and poor Bishop score.
Associated medical disorders observed were, anaemia in 84 (79%) patients, Diabetes mellitus in 8 (8%), Pregnancy induced hypertension in 8 (8%), Hepatitis C in 4 (4%) and Hepatitis B infection in 1 (1%). In anaemic women, haemoglobin concentration was less than 7 gm% in 31 (29%) cases and it could not be concluded whether anaemia was the cause or consequence, of of antepartum haemorrhage, as patients were un-booked with no antenatal record.
Table-1, shows maternal morbidity and mortality 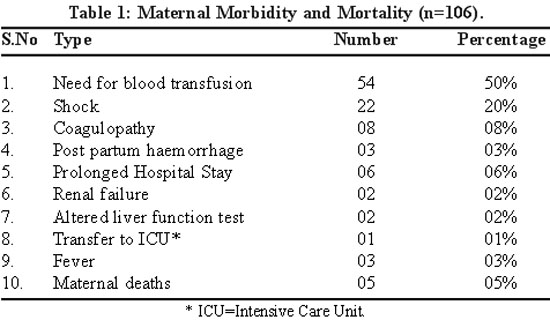
Table-2 shows perinatal mortality and morbidity in 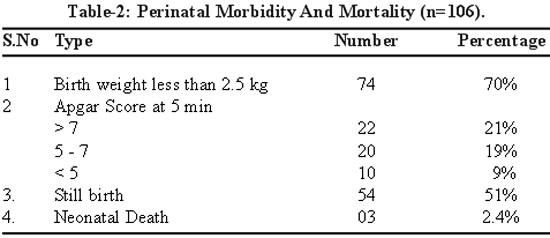
Discussion
An alarmingly high figure of abruption placenta was reported in our series in contrast to advanced countries, but conforming with various Pakistani studies.4-6 Liaquat University Hospital being the tertiary referral hospital with a large catchment area, drains mostly high risk cases.
Lack of antenatal care and rural residence were found to be the important risk factors in women suffering from abruptio placentae. Rural women are among the most disadvantaged people in
Availability and accessibility of antenatal care in remote areas will reduce the morbidity and mortality associated with abruptio placentae. It will provide advice on iron and folate supplementation, and to treat pre-existing medical conditions like anaemia, hypertension and diabetes mellitus. Pregnancy complications associated with abruptio placentae like gestational diabetes mellitus, and pre-eclampsia will be detected early and managed appropriately.
Another important risk factor found to be associated with this moribund condition was multiparity, a reflection of poor family planning practices in
Most of the patients in the study were anaemic (79%), a fact also highlighted by other published reports.5,10 World Health Organization considers anaemia as a moderate public health problem in Pakistan with the estimated prevalence of 39.1% (29.6-49.5%) in pregnant women. Many of these women enter pregnancy in an anaemic state as estimated prevalence of anaemia in non pregnant state is 27.9% (24.2-31.9%).11 Anaemia is the result of malnutrition especially proteins, zinc, iron and concurrent illnesses like malaria, diarrhoea and parasitic infestations. Anaemic patients are more prone to develop haemorrhage and its complications. Hypertension and Diabetes mellitus were other risk factors observed in our series. Several other studies also confirm this association.12-14 Hypertensive patients had three fold increased risk of placental abruption compared to normotensive patients.5 Hypertension and Diabetes mellitus can cause and enhance the placental insufficiency and ultimately lead to abruption.
Prematurity was found in 54% cases. This observation is also evident from other studies.15,16 Preterm deliveries, pregnancy induced hypertension, intrauterine growth restriction and abruptio placentae share the common etiological factors and the present study gave further insight into the problem.17
Caesarean section rate was quite high (27%) but in line with other Pakistani studies.18 In majority of the cases, Caesarean section was performed in foetal interest. Witlin and Sibai19 found that Caesarean delivery was associated with significant reduction in neonatal mortality. Maternal and foetal outcome can be optimized through attention to risk and benefits of conservative management versus expeditious delivery in cases of placental abruption.
Poor perinatal outcome characterized by high intrauterine deaths in our study is consistent with reports from public sector hospitals of
Conclusion
The frequency of abruptio placentae is alarmingly high with adverse maternal and foetal outcome. Multiparity, un-booked status, rural residence and maternal anaemia are important risk factors. Early intervention, expeditious delivery and strengthening of safe motherhood services particularly in rural areas, will help to prevent and reduce the gravity of the situation.
References
1.Deering S.H Abruptio placentae. (Online) 2007 (Cited 2007 June 2). Available from URL: http://emedicine.medscape.com/article/252810-overview.
2.Arulkumaran S, Symonds I, Fowlie A. ed. Oxford handbook of obstetrics and gynaecology. 2nd ed. New York: Oxford University Press, 2004.
3.Liaquat NF, Shoib T, Shuja S. A study of abruptio placentae. J surg Pakistan 2006; 11: 27-30.
4.Nizam K, Memon N, Laghari MS. Renal failure - A dreadful complication seen in patients with Abruptio placentae. Pak Armed Forces Med J 2004; 54: 84-7.
5.Jabeen M, Gul F. Abruptio Placentae Risk facots and perinatal outcome. J Postgrade Med Inst 2004; 18: 669-76.
6.Noorani KJ, Noorani M. Prevalence of acute renal failure in patients developing Abruptio Placentae as a consequence of PIH. Pak J Obstet Gynaecol 1995; 8: 15-6.
7.National Institute of Population Studies (NIPS) [Pakistan] and Macro International. 2008. Pakistan Demographic and Health Survey 2006-07: Key Findings. Calverton, Maryland, USA: NIPS and Macro International. (Online) (Cited 2009 May 11). Available from URL: http://www.measuredhs.com/pubs/pdf/SR142/SR142.pdf.
8.Bibi S, Memon A, Sheikh JM, Queshi AH. Severe acute maternal morbidity and intensive care in a public sector university hospital of Pakistan. J Ayub Med Coll Abbottabad 2008; 20: 109-12.
9.Bibi S, Memon A, Memon Z, Bibi M. Contraceptive knowledge and practices in two districts of Sindh, Pakistan: A hospital based study. J Pak Med Assoc 2008; 58: 254-8.
10.Ananth CV, Oyelese Y,Yeo L, Pradhan A, Vintzileos AM. Placental abruption in the United states, 1979 through 2001: temporal trends and potential determinants. Am J Obstet Gynecol 2005; 192: 191-8.
11.Benoist B, Mclean E, Egli I eds. Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia. World Health Organization, 2008. (Online) 2008 (Cited 2009 May 9). Available from URL: http://whqlibdoc.who.int/publications/2008/9789241596657_eng.pdf.
12.Dafallah SE, Babikir HE. Risk factors predisposing to abruptio placentae. Maternal and fetal outcome. Saudi Med J 2004; 25: 137-40.
13.Odendaal HJ, Hall DR, Grove D. Risk factors for and perinatal mortality of abruptio placentae in patients hospitalized for early onset severe preeclampsia: a case controlled study. J Obstet Gynaecol 2000; 20: 359-64.
14.Kyrklund Blomberg NB, Genser G, Cnattingius S. Placental abruption and perinatal death. Paediatr perinat Epidemiol 2001; 15: 290-7.
15.Rana A, Sawhney H, Gopalan S, Panigrahi D, Nijhawan R. Abruptio placentae and chorioamnionitis - microbiological and histological correlation. Acta Obstet Gynaecol Scand 1999; 78: 363-6.
16.Rasmussen S, Irgens LM, Dalaker K. Outcome of pregnancies subsequent to placental obruption: a risk assessment. Acta Obstet Gynaecol Scand 2000; 79: 496-501.
17.Rasumussen S, Irgens LM, Dalaker K. A history of placental dysfunction and risk of placental abruption. Paediatr Perinat Epidemiol 1999; 13: 9-27.
18.Sarwar I, Abbasi AN, Islam A. Abruptio placentae and its complication at Ayub Teaching Hospital Abbotabad. J Ayub Med Coll Abbottabad 2006; 18: 27-31.
19.Witlin AG, Sibai MB. Perinatal and maternal outcome following abrouptio placentae. Hypertens Pregnancy 2001; 20: 195-203.
20.Nayama M, Tamakloe-Azamesu D, Garba M, Idi N, Djbril B, Kamaye M et al. Abrouptio placentae. Management in a reference Nigerian maternity. Prospective study about 118 cases during one year. Gynecol Obstet Fertil 2007; 35: 975-81.
21.Thieba B, Lankonade J, Akotionga M, Kyelem C, Ouedraogo A, Ouerdraogo CM et al. Abruptio placentae: epidemiological, Clinical and prognostic aspects with respect to a 177 case series. Gynacol Obstet Fertil 2003; 31: 429-33.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: