
Ambreen Asad ( Army Medical College/NUST,Rawalpindi. )
Muhammad Amjad Hameed ( Islamic International Medical College,Rawalpindi. )
Umar Ali Khan ( Islamic International Medical College,Rawalpindi. )
Mujeeb-ur-Rahman Abid Butt ( Combined Military Hospital,Rawalpindi. )
Nadeem Ahmed ( Armed Forces Institute of Rehabilitation Medicine,Rawalpindi. )
Amina Nadeem ( Army Medical College/NUST,Rawalpindi. )
September 2009, Volume 59, Issue 9
Original Article
Abstract
Objective: To compare the nerve conduction studies in clinically undetectable and detectable sensorimotor polyneuropathy in type 2 diabetics.
Methods: Diagnosed diabetics (n=60) were divided in two groups. Group 1 (n1=30) with clinically undetectable and group 2 (n2=30) with clinically detectable Diabetic Polyneuropathy. Detection of the sensorimotor neuropathy was done according to Diabetic Neuropathy Symptom Score and Diabetic Neuropathy Examination scores. The simplified nerve conduction studies protocol was followed in recording amplitudes, velocities and latencies of minimum two (Sural, Peroneal) and maximum six i.e. three sensory (Sural, Ulnar, Median) and three motor (Peroneal, Ulnar, Tibial) nerves.
Results: The comparisons were done between different parameters of nerve conduction studies with the neurological scores in undetectable and detectable groups using Pearson's chi square test. The amplitudes, velocities, latencies, outcome and grading of neuropathy in nerve conduction studies when compared with neurological detection scores showed a significant relation in each group regarding evaluation (p=0.005, p=0.004, p=0.05, p=0.00001, p=0.003 respectively).
Conclusions: Diabetic Neuropathy Symptom Score and Diabetic Neuropathy Examination Score together can help in prompt evaluation of the diabetic sensorimotor polyneuropathy though nerve conduction study is more powerful test and can help in diagnosing subclinical cases (JPMA 59:594; 2009).
Patients and Methods
This comparative cross-sectional study was conducted in
All the diabetic patients were taken from the outpatient department of CMH,
Relevant complaints regarding neuropathy were noted. History of neuropathy was carefully taken to avoid inclusion of cases due to any other cause of neuropathy. The patients were booked on the basis of selection criteria. For inclusion, the patients had to be diagnosed type 2 diabetics between 25-61 years (male or female) with duration of known diabetes greater than one year and with intact and normal sites to be tested. If there was evident neuropathy, it had appeared after the onset of diabetes. All the patients with any other type of neuropathy, diagnosed or suspected, were excluded from the study. The patients with acute or chronic musculoskeletal disorder, poor compliance, pregnancy and taking drugs which may improve, mask or aggravate the normal course of neuropathy; for example pyridoxine, NSAIDS, metronidazole, hydralazine and isoniazid were excluded from the study.
The clinical neurological examination was conducted to confirm symmetrical diabetic neuropathy and then to grade it according to the scores mentioned. After examining 80 patients a total sample of 60 diagnosed type 2 diabetic patients (N = 60) were selected. The patients having clinically undetectable neuropathy were placed in group 1 (n1=30) and those found to have detectable neuropathy were placed in group 2 (n2=30) on the basis of DNS and DNE. The patients were checked on both sides for each score to confirm symmetry. They were labeled to have clinically detectable neuropathy if DNS was > 1 (max: 4) or DNE was >3 (max: 16). Undetectable neuropathy was labeled if DNS was < 1 or DNE was < 36. Blood sugar fasting was checked in all the patients with the help of glucometer (Ascensia Elite) by Bayer to assess the glucose level and control.
Nerve Conduction Studies were done at room temperature of 23 ± 2 ºC. For all studies, the machine used was Keypoint work station (
The simplified nerve conduction studies (NCS) protocol12 was followed which is as under:
1) Sural sensory and peroneal motor NCS were performed in one lower extremity. If both studies were normal, NCS was discontinued.
2) If sural sensory or peroneal motor NCS were abnormal, NCS of at least the ulnar sensory, median sensory, and ulnar motor nerves in one upper extremity were done.
3) If a response was absent for any of the nerves (sensory or motor), NCS of the contra lateral nerve was performed.
4) If a peroneal motor response was absent, an ipsilateral tibial motor NCS was performed.
All the data was recorded on pre designed questionnaire proforma which was later transferred to the SPSS version 10 for analysis.
Measuring the variables of NCS:
In all the six nerves amplitudes, velocities and latencies were individually assessed. They were assigned numerical grades of severity according to their values and then net score was assigned to each variable labeling them as normal or mild, moderate or severe neuropathy according to the average of 2 to six nerves2. Presence or absence of neuropathy was labeled as outcome. Overall score (grade) was assigned to NCS again as normal, mild, moderate or severe neuropathy according to the scores of amplitudes, velocities and latencies. All the scoring was done manually and later transferred to the computer.
Statistical Analysis
Pearson chi square test was used to compare the group 1 and group 2 with the findings of NCS. Amplitudes, velocities and conduction velocities, outcome (presence or absence of neuropathy) and grading (mild, moderate and severe neuropathy) all were compared in each group with the findings of the DNS and DNE to assess their evaluation of diabetic neuropathy.
Results
Sixty patients were evaluated, on the basis of presence or absence of complaints of peripheral neuropathy, family history of diabetes and history of drugs affecting neuropathy. In addition gender of patients was also calculated. In group 1 (n1=30) there were 11 (36.7%) males and 19 (63.3%) females and there were 13 (43.3%) males and 17 (56.7%) females in group 2 (n2=30). In group 1 the complaints of polyneuropathy were present in 7 (23.3%), family history was positive in 19 (63.3%) while drug history was positive in 3 (10%) patients. In group 2 the patients with polyneuropathy were 23 (76.7%), family history was positive in 14 (46.7%) while drug history was positive in 3 (10%).
When the different components of NCS were compared with the outcome of the neurological scores in each group the following results were obtained:
Amplitudes: The amplitudes when compared in group 1 and group 2 had a significant relation with neurological detection score regarding evaluation (p=0.005) as shown in Figure-1.
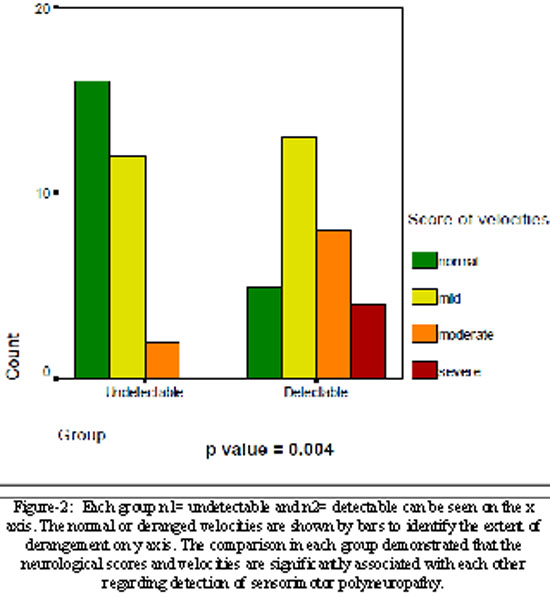
Velocities: The velocities when compared in each group indicated significance (p=0.004) as shown in Figure-2.
Latencies: The comparison of latencies in both the groups again had significance (p=0.05) as shown in Figure-3.
When total outcome (normal or abnormal in each group) of NCS was compared with the neurological scores it was again significantly (p <0.001) associated with each other regarding detection of sensorimotor polyneuropathy. It means 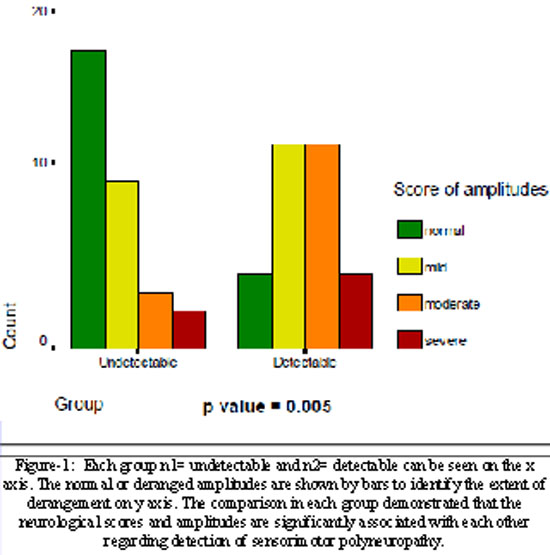
Similar results were found when grades of neuropathy were compared in each groups (p=0.003). The normal or 
Discussion
The detection and grading of diabetic neuropathy is an area of ongoing interest for the researchers and clinicians, not only for diagnosing and managing it earlier but also for understanding the disease which is still under exploration. Mostly nerve conduction studies have been accepted as an essential part of diagnosis for DPN as it has many benefits.13,14
When comparison of nerve conduction studies was done with detection scores in each group, though NCS detected more cases of neuropathy than the scores, there is significant association between clinical scores and NCS or its major components. The results and figures (1, 2 and 3) show that both clinical tests and NCS have a value in detecting cases of peripheral neuropathy. The NCS however is more powerful in detecting neuropathy which shows that NCS is helpful in detecting sub clinical neuropathies also.
Similar results have been obtained by most of the studies. A study in
In
Screening should be done on regular basis for sub clinical cases to avoid the complication as according to recent suggestions by American Diabetes Association the purpose of screening is to identify asymptomatic individuals who are likely to have diabetes or pre- diabetes. Separate diagnostic tests using standard criteria are required after positive screening tests to establish a definitive diagnosis.18
All the basic components of NCS were compared in each group. According to results, in all the components, amplitudes are the strongest measures of neuropathic problems and then are the other components. A latest study by Hsu WC et al.19 concludes that sural amplitudes and peroneal motor conduction velocities can be used as only markers for neuropathy. The same nerves were included in our study as initial screening for assessing nerve function.
Aring et al.20 concluded in a review that value of clinical examination has been recognized by different health care centers and there are suggestions to evaluate small nerve fibers with temperature, light, or pinprick testing and to test large nerve fibers by vibratory sensation, position sense, muscle strength and reflexes. Meijer et al.6 studied that role of basic test like tuning fork may still have better value than modern test like monofilament. It was concluded from this study that use of the 128-Hz tuning fork is a valid and reliable test for screening purposes and manageable in clinical practice. They claimed that the tuning fork deserves a central role in diagnosing diabetics for neuropathy. However its role was not compared with the nerve conduction studies for evaluation of patients. We also included tuning fork testing in our clinical scores but our results were different. Though vibration perception was impaired in some cases of neuropathy but we found that reflexes were lost in most patients with diabetic neuropathy in our population. So we believe that it is not the test of choice for detecting maximum cases of neuropathy.
Clinical examination can detect and grade neuropathy in majority of cases. However NCS was more powerful than any other test to detect the diseased cases in our study. Therefore we can use each, NCS or clinical examination for detecting and grading diabetic neuropathy and using both gives us a better chance for earlier diagnosis and more precise grading of neuropathy.
Conclusions
Diabetic Neuropathy Symptoms Score and Diabetic Neuropathy Examination Score can be used for prompt detection of neuropathy.
NCS is a more reliable tool for detection of diabetic sensorimotor polyneuropathy especially for the sub-clinical neuropathies. Routine NCS should be done on diabetics at least on yearly basis.
Introduction
The physiological properties of nerve and muscle are usually modified due to pathophysiological changes resulting from many diseases like diabetes.1 Diabetic sensorimotor polyneuropathy (DSPN), the most common complication of diabetes can be assessed clinically and electrophysiologically.2,3 The DSPN should be assessed independently and if assessed with other kinds of neuorpathies occurring in diabetes like compressive or truncal neuropathy, it may mask the individual evaluation of each kind.4 This is also supported by the fact that the DSPN can exist independently without involvement of autonomic neuropathy.5
There is a role for Diabetic Neuropathy Symptom (DNS) and Diabetic Neuropathy Examination (DNE) scores in detecting DSPN.6 Symptoms usually develop at any degree of neuropathic impairment or may not occur at all which indicates the need for doing nerve conduction studies (NCS).7 It has also been seen that abnormal changes in glucose levels do result in different types of nerve derangements including axonal injury or demyelination.8 The neuropathy, whether demyelinating or axonal, can be determined on the basis of nerve conduction studies.
The DSPN if diagnosed earlier by improving the already used methods in our set up can help to pick up those patients who are at risk of complications like foot ulcers which may eventually end in amputation.9 In many instances type 2 diabetes can be effectively treated, at least in the initial stages and the early and precise detection can help in better understanding the pattern of patho-physiological changes as well as in controlling crippling illness like peripheral neuropathy. 10,11
Reference
1.Krarup C. Nerve conduction studies in selected peripheral nerve disorders. Curr Opin Neurol 2002; 15: 579-93.
2.Feki I, Lefaucheur JP. Correlation between nerve conduction studies and clinical scores in diabetic neuropathy. Muscle Nerve 2001; 24: 555-8.
3.Bloomgarden ZT. Diabetic neuropathy.Diabetes Care 2008; 31: 616-21.
4.Low PA, Benrud-Larson LM, Sletten DM, Opfer-Gehrking TL,
5.Tentolouris N, Pagoni S, Tzonou A, Katsilambros N. Peripheral neuropathy does not invariably coexist with autonomic neuropathy in diabetes mellitus. Eur J Intern Med 2001; 12: 20-7.
6.Meijer JW, Bosma E, Lefrandt JD, Links TP, Smit AJ, Stewart RE, et al. Clinical diagnosis of diabetic polyneuropathy with the diabetic neuropathy symptom and diabetic neuropathy examination scores. Diabetes Care 2003; 26: 697-701.
7.Soliman E, Gellido C. Diabetic Neuropathy, eMedicine. [Online] 2009 [Cited 2004 Sept]. Available from URL: http://www.emedicine.com/NEURO.
8.Niazi PHK, Ahmad K, Hussain A, Butt AW, Alam A. Electrodiagnostic Evaluation of Diabetic Polyneuropathy. Pak Armed Forces Med J 2001; 51: 75-7.
9.Nelson EA, O'Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al. A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers. Health Technol Assess 2006; 10: iii-iv, ix-x, 1-221.
10.Dobretsov M, Romanovsky D, Stimers JR. Early diabetic neuropathy: triggers and mechanisms.World J Gastroenterol 2007; 13: 175-91.
11.Guyton AC, Hall JE. Text Book of Medical Physiology. 10th ed. Philadelphia; Pennsylvania: W.B. Saunders Company 2000.
12.England JD, Gronseth GS, Franklin G, Miller RG, Asbury AK, Carter GT, et al. Distal symmetric polyneuropathy: a definition for clinical research: report of the American Academy of Neurology, the American Association of Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 2005; 64:199-207.
13.Perkins BA, Bril V. Diabetic neuropathy: a review emphasizing diagnostic methods.Clin Neurophysiol 2003; 114: 1167-75.
14.Franssen H, van den Bergh PY. Nerve conduction studies in polyneuropathy: practical physiology and patterns of abnormality. Acta Neurol Belg 2006; 106:73-81.
15.Liu MS, Hu BL, Cui LY, Tang XF, Du H, Li BH. Clinical and neurophysiological features of 700 patients with diabetic peripheral neuropathy. Zhonghua Nei Ke Za Zhi 2005; 44:173-6.
16.Rota E, Quadri R, Fanti E, Poglio F, Paolasso I, Ciaramitaro P, et al. Clinical and electrophysiological correlations in type 2 diabetes mellitus at diagnosis. Diabetes Res Clin Pract 2007; 76:152-4.
17.Rota E, Quadri R, Fanti E, Isoardo G, Poglio F, Tavella A, et al. Electrophysiological findings of peripheral neuropathy in newly diagnosed type II diabetes mellitus. J Peripher Nerv Syst 2005; 10:348-53.
18.Standards of medical care in diabetes-2006.American Diabetes Association. Diabetes Care 2006; 29: S4-42.
19.Hsu WC, Chiu YH, Chen WH, Chiu HC, Liou HH, Chen TH. Simplified electrodiagnostic criteria of diabetic polyneuropathy in field study (KCIS No. 14). Neuroepidemiol 2007; 28: 50-5.
20.Aring AM, Jones DE, Falko JM. Evaluation and prevention of diabetic neuropathy. Am Fam Physician 2005; 71:2123-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: